

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The pigmented or melanotic variant of choroid plexus carcinoma (CPC) is very rarely encountered; the case presented herein is only the third reported case.1 The pigment granules in the tumor have properties of neuromelanin and lipofuscin.2,3 If the tumor is located in the posterior fossa, it needs to be distinguished from some of its close histologic mimics. Histopathological examination supported by immunohistochemistry helped the authors to diagnose this tumor. Some studies have demonstrated that complex cytogenetic studies aid its diagnosis.3
Case Report
An 11-year-old female child presented with headache, vomiting, and swaying toward the left while walking that first appeared 3 months previously, and diminished vision for the 15 days prior to admission. On neurological examination, the patient was conscious and responding to commands with sparse verbal output. She slept in the left lateral position throughout. Within 3 days of admission, she developed truncal ataxia, increasing salivation, difficulty in swallowing, and disorientation. The fundus could not be examined since the patient would not co-operate. These features led to the clinical diagnosis of posterior fossa lesion involving the left cerebellum.
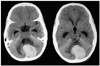
Computed tomography revealed a mass involving the fourth ventricle (Fig. 1). The operative finding was a grayish black, soft, friable, and ill-defined tumor arising from the fourth ventricle that infiltrated the left cerebellar hemisphere. The tumor was highly vascular and measured 3.5 cm across. Squash cytology revealed a malignant pigmented tumor. A suboccipital craniotomy and total tumor decompression were performed, and the mass was sent for histopathological analysis.
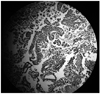
Examination of multiple hematoxylin-and-eosin-stained sections revealed a tumor containing monomorphic cells with abundant eosinophilic cytoplasm, round-to-oval irregular nuclei, and prominent nucleoli arranged predominantly in a papillary pattern, with focal solid areas. Dense intra- and extracellular melanin pigment was present. Mitotic activity was 7/10 in a high-power field. Focal areas of hemorrhage and necrosis were seen (Fig. 2). The pigment granules were positive for Fontana-Masson stain. An immunohistochemistry panel included HMB-45, cytokeratin, glial fibrillary acidic protein, S-100 protein, vimentin, synaptophysin, and carcinoembryonic antigen. The tumor was positive for cytokeratin, S-100 protein, and vimentin; a diagnosis of CPC was made. The patient could not be followed-up since she died 15 days after surgery.
Discussion
CPCs, which have a predilection for the posterior fossa, are rarely seen in children.4,5 The tumor constitutes only 0.4-0.6% of human intracranial tumors. Pigmented variants of CPC are rare, with only two other cases having been reported in the literature.1,4 The pigmented granules have the properties of neuromelanin and lipofuscin, and appear to be formed by "melanization" of lipofuscin, as proposed by Barden's theory of pseudoperoxidation.5
The differential diagnosis of the reported tumor includes pigmented papillary medulloblastoma of the cerebellum, pigmented ependymoma with papillae, and metastatic melanoma. Pigmented papillary medulloblastoma is a densely cellular tumor with an oval- to carrot-shaped nucleus, where the cells are arranged in rows and in gland-like clefts. In a few places the cells are arranged in a papillary pattern and contain pigment. The tumor tissue is immunopositive for cytokeratin, vimentin, and HMB-45, but also for epithelial membrane antigen.6 Ependymomas may also exhibit pigment. This type of tumor is densely cellular with perivascular rosettes and pseudorosettes, at places exhibiting a pseudopapillary pattern. The cells have a densely speckled nucleus, tapering cytoplasm, and a perivascular orientation of melanin. The tumor is positive for glial fibrillary acidic protein and HMB-45.7 Low-grade pigmented variants of CPCs contain predominantly a papillary pattern, and high-grade tumors have more solid areas. In the case reported herein, the tumor was a low grade.8
Very rarely, metastatic malignant melanoma may be considered in the differential diagnosis, but in our case there was no associated neurocutaneous syndrome. Staining for synaptophysin helps to distinguish this tumor from CPC and other metastatic papillary tumors.8
Recent cytogenic studies have revealed some chromosomal abnormalities associated with CPC, including gains of 1q, 4q, 10q, 14q, 20q, and 21q, and deletion of 5p, 9p, 15q, and 18q.9 CPCs are generally rapidly growing tumors with a poor prognosis. With the advent of specific immunohistochemical markers, optimal management requires the ability to differentiate pigmented variants of CPC from its histological and radiological mimics.
 XML Download
XML Download