

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sleep is a natural and inevitable part of human life. However, in about 2-5% of the adult population, sleep induces an unnatural and abnormal increase in upper-airways resistance, a condition known as obstructive sleep apnea (OSA).1,2 It has been shown that OSA can significantly and independently increase the risks of cardiovascular and cerebrovascular diseases.3 Oxidative stress, systemic inflammation, sympathetic activation, hemodynamic changes, and insulin resistance are the linking mechanisms between OSA and increased cardiovascular risk.3 Accelerated atherosclerosis and endothelial dysfunction also underlie this association.4,5
Endothelial microparticles (EMPs) are small (<1 µm) vesicles that are released from the endothelium in response to diverse stimuli including oxidative stress and inflammation.6 EMPs can be differentiated from other microparticles originating from leukocytes, erythrocytes, or platelets, and can be quantified by flow cytometry using specific antibodies raised against CD31 [platelet endothelial cell adhesion molecule (PECAM)], annexin-V, CD62E (E-selectin), or CD42 (platelet glycoprotein), because they carry cytoplasmic components and cell-surface antigens of endothelial origin.6 The level of circulating EMPs in peripheral blood is augmented in various conditions that render the patient prone to endothelial damage or atherosclerosis, such as cerebrovascular disease,7 hypertension,8 hypercholesterolemia,9 diabetes mellitus,10 smoking,11 and acute coronary syndrome.12 Therefore, EMPs are regarded as markers of vascular damage. Moreover, EMPs themselves might contribute to cardiovascular pathogenesis by affecting endothelial function, angiogenesis, and coagulation.13-15 Therefore, EMP levels are likely to be higher in OSA than in the non-OSA condition, and the difference may explain the link between OSA and cardiovascular diseases.
Endothelial progenitor cells (EPCs) are bone-marrow-derived circulating cells that act as an endothelial reservoir for replacing damaged or dysfunctional endothelium and counteracting ongoing injury.16 EPC levels are associated with cardiovascular diseases and can be used to predict future vascular events, in that lower levels are associated with poorer outcomes.16-18 Therefore, levels of EPC in OSA will be a reflection of the vascular status.
Two recent studies found no difference in EMP levels between OSA and non-OSA subjects.19,20 One of these studies included only minimally symptomatic OSA patients,19 and the other investigated subjects with both OSA and pulmonary hypertension.20 Therefore, it is difficult to generalize their results. On the other hand, studies of EPC in OSA have produced inconsistent findings.21-23
We measured the levels of EMPs and EPCs in OSA subjects and compared them to those measured in non-OSA subjects, and documented the changes in these levels after treatment. The tested hypothesis was that the levels of EMPs and EPCs differ between OSA and non-OSA, are correlated with OSA severity and carotid atherosclerosis, and change after treatment.
Methods
Subjects and assessment
Following Institutional Review Board approval, we prospectively recruited adults (≥20 years old) consecutively between March 2007 and March 2008 who had a history of habitual snoring or observed apneas. All subjects provided informed consent to participate in the study. We excluded subjects with any of the following conditions: central sleep apnea; other sleep disorders such as insomnia, restless legs syndrome, parasomnia, and narcolepsy or other hypersomnias; history of any cardiovascular, cerebrovascular, or pulmonary diseases; history of or laboratory-detected renal, hepatic, or hematologic disorder; clinical or laboratory evidence of inflammatory disease; history of autoimmune disease or malignancy; recent (within 4 weeks) trauma; history of migraine, thyroid disease, or psychiatric disorder; current use of vitamin or anti-inflammatory drugs such as aspirin; or an inability to understand the consent form.
Subjects underwent full-night diagnostic polysomnography (Comet XL Lab-based PSG, TWin PSG software, Grass-Telefactor, West Warwick, RI, USA) followed by standard scoring.24 Obstructive apnea was defined when there was an absence or reduction of airflow lasting more than 10 s with ongoing respiratory efforts, and hypopnea was scored as a reduction in airflow of at least 30% for more than 10 s with associated oxygen desaturation of more than 3%. The OSA diagnosis was based on an apnea-hypopnea index (AHI): those with AHI scores of at least 5 were was assigned to the OSA group, and the remainder were assigned to the OSA-free group. The OSA group was further subdivided into mild (AHI<15), moderate (AHI 15-30), and severe (AHI>30). AHI and minimum oxygen saturation were used as severity indices. Subjects with central sleep apneas, regardless of coexisting OSA, were excluded from the study.
Clinical evaluation was aided by a structured interview form, which included the Epworth Sleepiness Scale.25 The following clinical findings were documented as designated confounders: age, gender, body mass index (BMI), hypertension, diabetes mellitus, hyperlipidemia, current smoking, habitual alcohol drinking, and medication. Blood glucose and lipid levels were measured after fasting for at least 8 h. Systolic and diastolic blood pressures were measured three times with 10-min intervals between each, in the supine position at the sleep laboratory, after which, polysomnography was performed with the aid of a mercury sphygmomanometer. Hypertension was defined when the mean systolic pressure was more than 140 mmHg or the mean diastolic pressure was more than 90 mmHg, or the subject was on antihypertensive medication. Height and weight were also measured in the laboratory. A subject was defined as being overweight with a BMI of at least 23.0 kg/m2.26 Diabetes mellitus was defined when the subject had a relevant history or was on diabetes therapy. Hyperlipidemia was diagnosed when the total cholesterol level exceeded 240 mg/dL, when the low-density lipoprotein-cholesterol level exceeded 160 mg/dL, or when the subject was taking a lipid-lowering agent. Current smoking was defined when the subject was smoking or had smoked within 6 months prior to enrollment in the study. Males who consumed at least 4 units of alcohol per day and females who consumed at least 2 units per day were classified as 'habitual drinkers'.27
The carotid intima-media thickness (IMT) was measured (as a marker of atherosclerosis) in the morning after polysomnography using high-definition B-mode ultrasonography with a 10.0-MHz linear array transducer (10L5, Terason 2000, Terason Ultrasound, Burlington, MA, USA) by one of the investigators (K-H Ji) who was blind to other subject information. A longitudinal image of the distal common carotid artery was acquired. Measurements were performed 1 cm below the bifurcation at end-diastole in the segment including the thickest point, but not plaques, on the far wall using software calipers (Intimascope, Media Cross, Tokyo, Japan). The average IMT from both sides was recorded. The presence of plaques was documented in the exposed areas of the bilateral common, external, and internal carotid arteries, and bulbs. A plaque was defined as a localized thickening greater than 1.2 mm that did not uniformly involve the entire artery. The degree of plaque formation was defined as follows: 0=no plaque, 1=one small (<30% of the diameter), 2=one medium (between 30% and 50% of the diameter) or multiple small, and 3=one large (>50% of the diameter) or multiple with at least one medium. The presence of a plaque and its grade was also documented. IMT was measured in 80 subjects (76.9%); 24 subjects rejected the carotid study due to interference with their morning schedules.
Assay of EMPs and EPCs
In the morning (06:00-09:30 AM) after polysomnography, blood was drawn with a 21-gauge needle into heparinized bottles for EPC assay (25 mL) and citrated bottles for EMP assay (30 mL). The number of colony-forming units (CFU) on the cell culture was adopted as an EPC index. The method for CFU assay is described elsewhere.28
For EMP assay, whole blood was centrifuged at 1,500×g for 15 min and again for 2 min at 13,000×g to obtain platelet-poor plasma, which was then stored at -70℃ until the analysis. After 2-6 weeks, frozen samples were thawed in a 37℃ water bath for 5 min and then centrifuged at 3,000×g for 15 min. Prepared plasma (50 µL) was incubated at room temperature for 30 min with monoclonal antibodies (2 µL each) under gentle shaking (orbital shaker, 120 rpm). Circulating EMPs were quantified and differentiated from microparticles of other cellular origins by flow cytometry using a phycoerythrin-labeled CD31 (PECAM), allophycocyanin-annexin V, phycoerythrin-CD62E (E-selectin), and fluorescein isothiocyanate-CD42 (platelet glycoprotein; BD Biosciences, San Jose, CA, USA).6,29 Double labeling with CD42 was performed to exclude PECAM-positive (PECAM+) microparticles of platelet origin. Phosphate-buffered saline was added to a total volume of 1 mL and samples were analyzed on a FACS II flow cytometer (BD Biosciences) using the medium flow-rate setting and a 30-s stop time. Microbeads from a FACS Size Calibration Kit were used (Invitrogen, Carlsbad, CA, USA). EMPs of less than 1 µm were quantified as counts per microliter in specific populations of PECAM+CD42-negative (CD42-), PECAM+ annexin V-positive (annexin V+), and E-selectin-positive (E-selectin+) EMPs. Laboratory personnel were blinded to other data.
OSA intervention and follow-up analysis
Subjects who agreed to continuous positive airway pressure (CPAP) therapy underwent manual titration to normalize flow and sleep, including an AHI of <5/h. Titration was performed on a separate night. After CPAP therapy for 4-6 weeks, blood sampling for EPC and EMP analysis was performed in the morning (06:00-09:30 AM), and efficacy and compliance data were analyzed (S8 Elite and Autoscan 5.7, ResMed, Bella Vista, NSW, Australia). Changes in medications, alcohol consumption, smoking, Epworth Sleepiness Scale, BMI, and blood pressure were noted. We included only CPAP-treated subjects, because surgery has a relatively poor and inconsistent outcome, and any procedure per se might bias EPC and EMP profiles.30
Statistical analysis
All results are presented as mean±standard deviation or median (interquartile range) values for continuous variables, or number (percentage) values for categorical data. Variables not conforming to a normal distribution were log-transformed (EMPs), square-root transformed (AHI), or logit-transformed (minimum oxygen saturation) to achieve normality. Two-tailed Student's t-test and Pearson's chi-square (or Fisher's exact) test were adopted for group comparisons. The Mann-Whitney U (or Kruskal-Wallis Analysis of Variance) test was applied in the subgroup analysis.
The existence of correlations between OSA severity and outcome measures (EMPs, EPC index, IMT) was assessed using Pearson's correlation analysis. Treatment responses of EMPs and EPC index were tested by paired t-test. Multiple regression analysis used IMT, EPC index, or EMPs as dependent variables. Covariates were waist circumference, hyperlipidemia, alcohol drinking, and OSA severity indices. The absence of multicollinearity was checked using the variance-inflation factor. Statistical analysis was performed using SPSS software [SPSS 12.0 (SPSS Inc, Chicago, IL, USA)]. The null hypothesis was rejected at p<0.05.
Results
We evaluated 185 subjects consecutively; 49 were excluded due to cardiovascular diseases (n=23), vitamin intake (n=15), migraine (n=6), central apnea (n=4), and other factors (n=11). Seven had two or more of the exclusion conditions and 23 declined to participate; 113 were initially enrolled into the study. Of these, 92 were diagnosed as suffering from OSA. Blood sampling was unsuccessful or rejected in seven of these, and samples clotted in two. Ultimately, 104 subjects (age 40.8±10.1 years, 90.4% males, BMI 26.1±3.4 kg/m2) were enrolled in the study, of whom 82 were assigned to the OSA group and 22 to the non-OSA group.
EPC and EMP profiles
The OSA and non-OSA groups were balanced in terms of the distribution of key confounders (Table 1) and there was no significant difference in medication profiles, including antihypertensives (22.0% in OSA vs. 9.1% in non-OSA; p=0.94) and statins (8.5% vs. 4.5%, p=1.00). Of the 23 subjects taking antihypertensive drugs, 15 were single-drug users and 7 were taking 2 drugs; only 1 subject was taking 3 drugs. Statins were taken by seven of the OSA subjects, and fibric acid by one. One non-OSA subject was on a statin. Scores on the Epworth Sleepiness Scale were higher in the OSA group, in which the levels of PECAM+CD42-, PECAM+annexin V+, and E-selectin+ EMPs were also significantly higher than those in the non-OSA group (Table 1). There was a significant correlation between the levels of PECAM+CD42- and PECAM+annexin V+ EMPs (r=0.89, p<0.001), but not with those of E-selectin+ EMPs. The EPC index did not differ between the two groups (Table 1). The EPC index was lower in subjects on antihypertensive medication (32.9±22.1 vs. 45.6±25.4 for the OSA and non-OSA groups, respectively; p=0.03). However, antihypertensive medication had no effect on EMP levels. There was no association between statin medication and gender, or between EPC index and EMPs. IMT was measured in 18 (81.8%) non-OSA subjects and 62 (75.6%) OSA subjects (p=0.54), and was found to be greater in the latter (p=0.01)(Table 1).
While the OSA and non-OSA groups were balanced (Table 1), matching did not eliminate the time factor or the vascular remodeling that had resulted from coexisting conditions. Therefore, we performed subgroup analysis. Nineteen subjects (14 OSA, 16 males, 41.1±9.9 years old, BMI 25.1±3.1 kg/m2) were free from smoking, hypertension, hyperlipidemia, and diabetes mellitus.
The age, BMI, and gender did not differ between the OSA and non-OSA subjects. The levels of PECAM+CD42- EMPs were higher in OSA than in the non-OSA condition [150 (133-243) vs. 69 (33-102), respectively; p= 0.03]. However, the EPC index score (p=0.30) and levels of PECAM+annexin V+ (p=0.09) and E-selectin+ EMPs (p=0.16) did not differ between the two groups.
Correlations between OSA severity, endothelial markers, and atherosclerosis
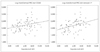
The levels of PECAM+CD42- and PECAM+annexin V+ EMPs differed among mild, moderate, and severe OSA subjects, as did BMI and the proportions of hyperlipidemia and habitual alcohol drinking (Table 2). However, the levels of E-selectin+ EMPs and EPC index were not affected by the severity of OSA. Levels of PECAM+CD42- and PECAM+ annexin V+ EMPs were positively correlated with AHI (Fig. 1), but not with age, BMI, blood pressure, glucose, or lipid levels (p>0.05). Logit-transformed minimum oxygen saturation was also correlated with PECAM+annexin V+ EMP level (r=0.23, p=0.04), but not with levels of PECAM+CD42- (r=0.19, p=0.09) or E-selectin+ EMPs (r=0.03, p=0.78), or with CFU (r=0.09, p=0.45). Multiple regression analysis revealed that AHI was significantly associated with PECAM+CD42- (p=0.02) and PECAM+annexin V+ EMP levels (p=0.004). BMI, hyperlipidemia, and alcohol drinking did not predict EMP levels. There was no collinearity among AHI and its covariates (variance-inflation factor <4.0). The arousal index was not correlated with either EMP level or EPC index (p>0.05).
The relationship between IMT and OSA severity, EPC index, and EMPs was assessed. Carotid Doppler ultrasound study was performed in 18 (81.8%) non-OSA subjects and in 62 OSA subjects: 16 (88.9%) with mild OSA, 10 (62.5%) with moderate OSA, and 36 (75.0%) with severe OSA. IMT was correlated with AHI with minimum saturation (r=-0.56, p<0.001) and the levels of PECAM+CD42- and PECAM+ annexin V+ EMPs (Fig. 2). Multiple regression analysis revealed that AHI and minimum saturation independently explained the change in IMT (p<0.001). Furthermore, the correlation between IMT and levels of PECAM+CD42- and PECAM+ annexin V+ EMPs was independent of other confounders (β=0.059, SE=0.027, and p=0.03; and β=0.061, SE=0.023, and p=0.01; respectively). However, neither the EPC index nor the levels of E-selectin+ EMPs was correlated with IMT. Carotid plaques were observed in 15 subjects, of which 11 were grade 1 (1 non-OSA; 3 with mild, 1 with moderate, and 6 with severe OSA) and 4 were grade 2 (all with severe OSA). The frequency of occurrence of a plaque did not differ among non-OSA (5.6%), mild-OSA (18.8%), moderate-OSA (10.0%), and severe-OSA (27.8%) subjects (p=0.42), and was not associated with either EMP level or EPC index (p>0.05).
Endothelial markers after treatment
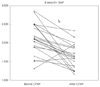
Twenty-one patients (25.6%) consented to CPAP therapy, during which one quit smoking. All other conditions were similar to those measured at baseline. Compliance was 89.3±7.1% (percentage of days with CPAP used for more than 4 h) and the median number of used-hours was 5.83±1.10 h. The mean levels of E-selectin+ EMPs decreased from 133/µL (range 79-311/µL) to 44/µL (25-77/µL) (p<0.001), but there were no significant changes in the EPC index or in the levels of PECAM+CD42- or PECAM+annexin V+ EMPs (Fig. 3) (Table 3). There was no correlation between levels of E-selectin+ EMPs and residual AHI. CPAP compliance did not affect the treatment response of EPC index and EMP level. In two subjects, levels of E-selectin+ EMPs increased (from 33/µL to 40/µL, and from 21/µL to 92/µL); the residual AHI was 1.60 and 2.90, respectively, and the number of used-hours was 5 h 26 min and 6 h 15 min, respectively. No change was noted in any of the other parameters.
Discussion
The study findings can be summarized as follows: 1) EMP levels were higher in OSA than in non-OSA subjects, but the EPC index did not differ, 2) the EMP level (PECAM+CD42-, PECAM+ annexin V+) was correlated with AHI, 3) the carotid IMT was parallel with OSA severity, and with levels of PECAM+CD42- and PECAM+annexin V+ EMPs, and 4) CPAP treatment reduced the levels of E-selectin+ EMPs.
Endothelial damage is one of the linking mechanisms between OSA and cardiovascular diseases.31 The present study found that overproduced EMPs and a thick IMT supports the endothelial pathology observed in OSA. The release of microparticles is triggered by various activating or apoptotic signals including cytokines, toxins, hypoxia, or shear stress.6 In OSA, repetitive cycles of hypoxia and reoxygenation causing oxidative stress are cues for EMP release. A high oxidative stress state has been documented in OSA, and it can be normalized by effective CPAP treatment.32-34 Moreover, OSA leads to systemic inflammation, as evidenced by increased levels of inflammatory mediators or cytokines, such as of tumor necrosis factor-α, interleukin-6, C-reactive protein, nuclear factor-κB (which is a proinflammatory transcription factor), and adhesion molecules including intercellular adhesion molecule-1 and E-selectin.5,34-36 Inflammation plays a central role not only in the development of atherosclerosis, but also in the formation of EMPs.6,37,38 This explains the significant correlations between OSA severity and levels of PECAM+ CD42- and PECAM+annexin V+ EMPs, and carotid IMT. E-selectin+ was also higher in the OSA group. The role of OSA in the production of EMPs was also supported by the subgroup analysis in subjects free from other vascular risk factors. Levels of PECAM+CD42- EMPs were higher in OSA subjects than in non-OSA subjects. However, the small sample may have been responsible for the absence of statistically significant differences in the other EMP levels.
A different subset of antigen expressions on EMPs in vitro was documented depending on the stimulus type (i.e., apoptotic or activation).39 Destructive injury, as an apoptotic signal, induced the expression of PECAM+CD42- and PECAM+ annexin V+ EMPs, and tumor necrosis factor-α, as an activating signal, increased that of E-selectin+ EMPs.39 A potential difference in the biologic significance of EMP subtypes was suggested.40,41 In this study, levels of PECAM+CD42- EMPs were correlated with those of PECAM+annexin V+ EMPs (r=0.89, p<0.001), suggesting a common pathophysiology-apoptosis. Endothelial apoptosis in OSA was demonstrated previously by measuring circulating apoptotic endothelial cells.42 Furthermore, the levels of PECAM+CD42- and PECAM+ annexin V+ EMPs paralleled the degree of atherosclerosis revealed by measuring carotid IMT (Fig. 2). Our findings suggest that OSA contributes to endothelial apoptosis and eventually predisposes to atherosclerosis.
Levels of E-selectin+ EMPs were higher in OSA but were not correlated with OSA severity (Table 1 and 2). The plateauing of E-selectin+ EMP levels may explain the lack of correlation. The dose-dependency between soluble plasma E-selectin and severity indices was not consistent in a previous study.43 However, the reduction in E-selectin+ EMP levels after CPAP supports the idea that OSA has a significant impact on it. As with E-selectin+, levels of soluble E-selectin reduced after CPAP.44 A reversible change in EMP levels was documented in both in vitro and in vivo studies.11,45 The temporary change in EMP levels and flow-mediated dilatation effected by a brief exposure to second-hand smoking supports not only its reversibility, but also its correlation with endothelial function.11
CPAP only reduced E-selectin+ EMP levels. Neither PECAM+ nor annexin V+ EMPs levels were altered by CPAP therapy lasting more than 4 weeks, with a residual AHI of less than 10. Although the metabolism of various EMPs is unclear, a longer half-life or a decreased clearance may contribute to persistently high PECAM+ and annexin V+ expressions. Follow-up after prolonged (>6 weeks) treatment may provide an explanation for this. Moreover, coexisting vascular risk, especially being overweight, might contribute to the resistant overproduction of other EMPs. With regard to metabolic syndrome, levels of PECAM+ and annexin V+ EMPs were higher in OSA subjects than in non-OSA subjects, whereas those of E-selectin+ EMPs were not.41 Uncontrolled metabolic factors may underlie the dissociated CPAP response. BMI and blood pressure, which are major factors of metabolic syndrome, did not change significantly after CPAP therapy (Table 3). Regardless of the dissociation, reducing the expression of E-selectin+ may afford further vascular protection, because EMPs themselves are known to have an impact on endothelial function, coagulation, and inflammation.13-15
A recent study found no difference in the level of PECAM+ CD41- expression between OSA subjects and the matched-controls.19 The subjects included in that study were less sleepy. Nonsleepy OSA differs from sleepy OSA, but the mechanisms underlying this condition are unclear.46 CPAP exerts a less favorable effect on nonsleepy OSA.47,48 In contrast, sleepiness is a predictor of blood pressure lowering and insulin resistance.49,50 Therefore, the EMP levels measured in this study would better represent the situation in real-life OSA.
EPC index was not different between OSA and non-OSA subjects, and was unaffected by treatment. Two previous studies were unable to document a difference in the EPC level between OSA and control subjects.21,23 Although EPC levels are inversely correlated with cumulative cardiovascular risk, circulating EPC levels are known to change in a time-dependent manner.16,51 Acute vascular events initiate the recruitment of EPCs from the bone marrow, but EPC levels normalize in the chronic phase.51 OSA is a chronic condition, and hence EPC levels might not differ between OSA and non-OSA subjects. Furthermore, coexisting vascular risk factors in both groups may have a more prominent effect on EPC level.
Our study had several limitations. Strictly speaking, as controls, the non-OSA group was not a predefined matched control from the general population, but rather constituted a group of subjects who had primary snoring without significant apneas on polysomnography. This may have biased the results. In addition, the treatment response was not addressed in a randomized fashion, but was only observed in a small (25.6%) proportion of subjects, because the Korean National Insurance scheme does not reimburse for CPAP therapy. Another limitation is that the measurement of EPC has not yet been standardized. EPC can be measured by flow cytometry or cell culture.52 The number of CFU in cell cultures has been shown to be related to the cumulative vascular risk.16,17 However, there is emerging evidence that EPCs defined by this method are not sufficient to give rise to an endothelial progeny.52 Although this study is the first to measure EPC levels with CFU, we cannot draw a firm conclusion about the involvement of EPCs in OSA. One study has demonstrated a reversible increase in EPC levels in OSA after CPAP treatment using flow cytometry.22 We have documented the overproduction of EMPs, which reflects the endothelial damage observed in OSA. Moreover, levels of apoptotic EMPs were correlated with carotid atherosclerosis, and CPAP therapy reduced E-selectin+ expression. Based on these findings, we conclude that endothelial damage is a linking mechanism between OSA and accelerated atherosclerosis, and that CPAP therapy may be effective in reversing endothelial activation and removing the undesirable effects of EMPs.




 XML Download
XML Download