

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The suicide rate in Korea in 2008 was reported to be 26.1 per 100,000 persons by the World Health Organization, which at the time was the highest among the Asian countries.1 People who commit suicide in Korea have various medical or psychiatric diseases.2 The most common comorbidity is depression (49%), followed by medical or surgical diseases (26%), schizophrenia (10%), dementia (6%), bipolar disorders (4%), mental retardation (3%), neurosis (1%), and alcoholism (1%). Although no data are available in Korea, the risk of suicide or suicide attempt is reportedly higher in people with epilepsy (PWE) than in the general population. Two large meta-analyses of 29 studies comprising 50,814 PWE concluded that suicide is more frequent in PWE than in the general population.3 A population-based, case-control study found that the risk of suicide was three times higher in PWE than in people with no such history.4 A questionnaire study from Canada found that the lifetime prevalence of suicidal ideation was higher in PWE (25%) than in people without epilepsy (13%).5
Various psychiatric comorbidities, including depression and anxiety, are known to be primary risk factors for suicide in both the general population and PWE.4,6-8 However, additional risk factors should be considered in PWE due to the impact of seizure-related factors on suicide. The degree of suicidality associated with simple partial seizures, primary generalized seizures, and secondary generalized seizures was found to be higher than that of complex partial seizures, and temporal lobe epilepsy in males represents a risk factor for suicidal behavior.9 Furthermore, a high frequency of seizures, independent of seizure type, is a risk factor for suicide,7 and concomitant use of phenobarbital increases the degree of suicidality in females.9 Cognitive deterioration and abnormal personality traits due to frequent seizures have been reported to increase the risk of suicide.10 Early age of epilepsy onset, high seizure frequency, and antiepileptic drug (AED) polytherapy are also risk factors for suicide.7 In addition to the seizure-related factors, the psychosocial factors for suicide including family issues, life stress, physical health, previous suicide attempt, and access to firearms should also be considered as risk factors for suicide.6,11 Furthermore, it is very important to know which factor most influences suicidal behavior. For example, if this was a seizure-related factor, we should treat epilepsy itself in order to prevent suicide. Conversely, if this was a psychiatric factor, we should focus on managing a patient's psychiatric problems rather than treating his or her epilepsy or psychosocial problems.
Predicting suicide is very difficult. Suicidal ideation is a common medical term for thoughts about suicide, which may be as detailed as a formulated plan but without the suicidal act itself. Suicidal ideation appears to be an important marker for identifying patients at risk of suicide12 and suicide attempts.13 Although most people who experience suicidal ideation do not commit suicide, it may be a significant warning sign for suicide attempts, especially in high-risk populations such as PWE.6 Therefore, the identification of risk factors for suicidal ideation may be critical for preventing PWE from committing or attempting suicide.
Once the suicidal risk has been assessed, it is important to determine the severity of that risk. According to Jacobs et al.14 at this stage it is important to conduct a "suicide inquiry" that includes direct questions about suicide ideation, presence or absence of a plan, and prior attempts. It is important to assess the types of thought that are occurring (e.g., active or passive), the frequency and persistence of those thoughts, and the factors that stop the person from following through with the suicide.14,15 Although there are simple methods that can be used to screen for suicidal ideation, such as the suicidality module of the Mini-International Neuropsychiatric Interview16 and the suicide item (question 9) of the Beck Depression Inventory (BDI),17 their simplicity (i.e., all or nothing assessment) makes them unsuitable for measure the severity of suicidal ideation. On the other hand, the Scale for Suicide Ideation-Beck (SSI-Beck) is a useful 19-item, self-reported questionnaire designed to detect and measure the severity of a patient's specific attitudes, behaviors, and plans to commit suicide.18 Although epileptic, psychiatric, and psychosocial factors have been related to suicide or suicide attempt in PWE, no studies have evaluated predictors for the severity of suicidal ideation-a warning sign for suicide attempt-in PWE. Therefore, we measured the severity of suicidal ideation in PWE and determined its risk factors. We also investigated the role of seizure-related variables in suicidal ideation, since some of those variables are treatable, and can thereby lessen the risk of suicidal behavior.
Methods
Subjects and study design
The study included 257 consecutive PWE who were medicated with AEDs and attended our epilepsy clinic between April 1, 2007 and October 31, 2009. We excluded patients who had undergone epilepsy surgery, and who had severe psychiatric or medical disorders, progressive neurological disorders, head injury, mental retardation (Korean-Wechsler Adult Intelligence Scale IQ <70),19 or alcohol or drug abuse. At enrollment, all subjects completed reliable and validated self-reported health questionnaires, including the BDI,20 Beck Anxiety Inventory (BAI),21 Symptom Checklist-90-Revised (SCL-90-R),22 and SSI-Beck.23 The subjects provided informed consent to participate in the study prior to completing the questionnaires. Demographic and clinical data were collected by interview and from information given in the patient's epilepsy diary. Seizure-related factors, such as seizure type, epilepsy syndrome, age at onset, duration of epilepsy, seizure frequency, duration of AED intake, number of AEDs, history of febrile convulsion, family history of epilepsy, and abnormalities on MRI and EEG were included.
We divided the PWE into the following three groups to determine the seizure frequency:
Drug-refractory epilepsy (DRE): defined as a failure of two or more AEDs and a seizure frequency of at least once per month for the previous 6 months before enrollment.
Well-controlled epilepsy (WCE): defined as a freedom from seizures for the previous year.
Poorly controlled epilepsy (PCE): defined as a seizure recurrence during the previous year, but not satisfying the criteria of DRE.
We also divided PWE into two groups according to the use or nonuse of γ-aminobutyric acid (GABA)-ergic AEDs. Since GABAergic AEDs are known to elicit depressive symptoms,24 we compared SSI-Beck scores between patients receiving GABAergic drugs and those not receiving GABAergic drugs. Valproate, topiramate, phenobarbital, clonazepam, vigabatrin, and gabapentin are classified as GABAergic AEDs according to the literature of Ketter et al.25 We compared demographic and clinical variables, and BDI, BAI, and SCL-90-R scores with the SSI-Beck scores, and used the findings to determine the risk factors for suicidal ideation. We also investigated the impact of seizure-related variables on those risk factors.
Questionnaires
BDI and BAI
The BDI is the most commonly used self-rating scale for depression.20 It comprises 21 items, each of which is scored on a scale of 0-3 according to how the patient feels at the current time. The BDI has been found to be strongly correlated with other ratings of depression, such as the Hamilton Depression Scale used by psychiatrists to rate depression. The BAI is a 21 item self-reported measure of anxiety severity.21 The scale consists of 21 items, each describing a common symptom of anxiety. The respondent is asked to rate how much he or she has been bothered by each symptom during the previous week, also on a 4-point scale ranging from 0 to 3. The Cronbach's alpha coefficients were 0.89 for BDI and 0.91 for BAI.
SCL-90-R
The SCL-90-R is a self-rated scale that has 9 psychiatric symptom domains, comprising 90 items with a rating scale with 5 degrees of severity.22 The psychiatric domains evaluated are somatization (alpha=0.72), obsessive-compulsive (alpha=0.83), interpersonal sensitivity (alpha=0.84), depression (alpha=0.89), anxiety (alpha=0.86), hostility (alpha=0.68), phobic anxiety (alpha=0.81), paranoid ideation (alpha=0.69), and psychoticism (alpha=0.67). The SCL-90-R index and symptom-scale scores are represented as T-scores, with a mean of 50 and a standard deviation of 10. Higher T-scores reflect a greater number and/or severity of a patient's self-reported symptoms.
SSI-Beck
The SSI-Beck is a 19-item, self-reported measure designed to evaluate the current severity of a patient's specific attitudes, behaviors, and plans to commit suicide.18,23 The items are rated on a 3-point scale from 0 to 2. The total score can range from 0 to 38, with higher scores indicating more intense levels of suicidal ideation. Cronbach's alpha coefficients were 0.87 for subjects of the study of Korean version of SSI-Beck23 and 0.82 for those of our study.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS version 17.0, SPSS Inc, Chicago, IL, USA). Descriptive statistics are presented in terms of counts, percentages, and mean±standard deviation values. The Mann-Whitney U-test or Kruskal-Wallis test for independent samples was applied to elucidate the differences in SSI-Beck scores according to seizure type, EEG and MRI abnormalities, psychiatric history, seizure frequency, and number of AEDs. We used simple linear correlations to evaluate the relationship between SSI-Beck scores and duration of education, IQ, and BDI, BAI, and SCL-90-R scores. Finally, a stepwise multiple linear regression analysis was used to study the multivariate relationships between covariables and SSI-Beck and BDI scores. Dummy coding was used for independent variables. Epilepsy syndrome, seizure frequency, and number of AEDs were categorized as three groups. The level of statistical significance was set at p<0.05.
Results
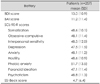
The demographic and clinical characteristics of the 257 PWE enrolled in this study (age 35.1±12.5 years, 60% males) are listed in Table 1. The duration of education was 12.8±3.0 years, and the IQ of the cohort was 103.3±15.5.
Regarding seizure type, 181 patients (70%) suffered from partial seizure and 76 patients (30%) from generalized seizure. The most common epilepsy syndrome was temporal lobe epilepsy. The age at onset and duration of epilepsy were 23.9±13.4 years and 11.2±9.3 years, respectively. Regarding seizure frequency, the proportions of WCE, PCE, and DRE were 51%, 21%, and 28%, respectively. Concomitant medical diseases were found in 15% of patients. The incidences of previous history of psychiatric diseases and febrile convulsion were 15% and 18%, respectively. The prevalence of a family history of epilepsy was low. The proportions of abnormal MRI and EEG findings were similar. The duration of AED intake was 8.5±8.3 years, and the number of AEDs being used per patient was 1.4±0.6; 32% of patients took AEDs with a GABAergic profile.
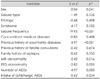
The scores of the entire cohort (i.e., n=257) for the various psychometric tests are listed in Table 2, and a comparison of the categorized variables among the demographic and clinical characteristics with the SSI-Beck score is given in Table 3. The SSI-Beck score was significantly correlated with sex (p=0.041), seizure frequency (p<0.001), previous history of psychiatric diseases (p<0.001), MRI abnormality (p=0.016), and EEG abnormality (p=0.005). The continuous variables are compared with the SSI-Beck score in Table 4. The duration of education (r=-0.13, p=0.032), IQ (r=-0.24, p<0.001), BDI score (r=0.7, p<0.001), BAI score (r=0.57, p<0.001), and nine domains of SCL-90-R [i.e., somatization (r=0.49, p<0.001), obsessive-compulsive (r=0.56, p<0.001), interpersonal sensitivity (r=0.62, p<0.001), depression (r=0.68, p<0.001), anxiety (r=0.61, p<0.001), hostility (r=0.64, p<0.001), phobic anxiety (r=0.51, p<0.001), paranoid ideation (r=0.57, p<0.001), and psychoticism (r=0.63, p<0.001)] were significantly correlated with SSI-Beck score.
The predictors of suicidal ideation as revealed by a stepwise multiple linear regression analysis of our findings are listed in Table 5. The strongest predictor of the SSI-Beck score was the BDI score (β=0.41, p<0.001), followed by several domains of SCL-90-R, such as obsessive-compulsive (β=-0.39, p<0.001), depression (β=0.38, p<0.001), hostility (β=0.22, p=0.002), paranoid ideation (β=0.17, p=0.01), and IQ (β=-0.10, p=0.017). These variables explained 59% of the variance in the SSI-Beck score.
Seizure-related variables determining the BDI score revealed by a stepwise multiple linear regression analysis are listed in Table 6. The strongest predictor of the BDI score was seizure frequency (β=0.21, p=0.004), followed by duration of education (β=-0.17, p=0.003), MRI abnormality (β=0.17, p=0.004), and number of AEDs (β=0.14, p=0.042). These variables explained only 18% of the variance in the BDI score.
Discussion
Suicide appears to be a particularly serious among people with chronic epilepsy who require treatment in specialty clinics.26 A case-control study of adults who had been hospitalized with epilepsy found a ninefold increase in risk of suicide with psychiatric comorbidity and a tenfold increase in relative risk with the use of antipsychotic drugs.7 In a cross-sectional study among 139 outpatients followed in 5 tertiary epilepsy centers in the United States, the highest risks for a suicide were associated with lifetime histories of major depressive episodes and manic episodes; a lifetime history of a mood and/or anxiety disorder was found to be significantly associated with the risk of suicidal ideation.6 A population-based study of suicide victims over a 15-year period in northern Finland suggested that suicide victims with epilepsy had suffered significantly more often from psychiatric disorders in their lifetime compared with those without epilepsy.8 A large, case-control study in Denmark, using five nationwide registries to obtain information about epilepsy, cause of death, psychiatric diagnoses, socioeconomic data, and demographic data, demonstrated that psychiatric history was a strong risk factor for suicide, even after adjusting for socioeconomic factors, and that affective disorder was the most common psychiatric disorder associated with the risk of suicide.4 Although we did not evaluate the predictors of suicide or suicide attempt, we found that the severity of suicidal ideation was also strongly correlated with BDI scores and other psychiatric symptoms.
Seizure-related variables including seizure type, epilepsy syndrome, seizure frequency, onset of epilepsy, and AED polytherapy have been reported to predict suicidality in PWE.7,9 However, there is a lack of available data on the psychiatric impact on seizure-related variables9 and only a weak association between seizure frequency or AED polytherapy and suicidality has been reported,7 and thus it has not been possible to explain the role of seizure-related variables on suicidal behavior. Our data also revealed that seizure-related variables are not major risk factors for suicide as well as depressive symptoms in PWE. Although the individual influence of seizure-related variables on suicidality is small, we should consider that these variables might together contribute to eliciting suicidal ideation. Seizure severity, as measured by assessing seizure frequency, type, duration, postictal events and duration, the occurrence of injuries, automatism, seizure clusters, warnings, tongue biting, incontinence, and overall functional impairment, was strongly correlated with the level of depression.27 Therefore, further studies are needed to evaluate the effects of seizure severity on suicidal behavior.
It has been suggested that AEDs are involved in the increased risk of suicidal behavior in PWE. GABAergic drugs including vigabatrin, tiagabine, topiramate, and phenobarbital can reportedly provoke or exacerbate depressive symptoms.24 The risk of developing major depressive disorders and suicidal ideation is higher in children taking phenobarbital than in those taking carbamazepine.28 However, we were unable to demonstrate a harmful effect of GABAergic AEDs on suicidal ideation. This can be explained by the involvement of valproate, a known mood-stabilizing agent,24,25 as a GABAergic AED. In our study valproate was used by as many as 42% of our patients, which may have attenuated the overall effect of GABAergic AEDs on mood or suicidal ideation. Although we did not demonstrate a harmful effect of AEDs on suicidality, the United States Food and Drug Administration (FDA) recently issued a warning regarding AEDs and suicidality.29 A meta-analysis of data from placebo-controlled trials with 11 different AEDs demonstrated that the odds ratio for suicidal ideation or behavior in the drug arms was 1.8 (95% CI, 1.24-2.66). Although the FDA alert raises potential problems regarding study interpretation due to methodological difficulties and the lack of information regarding the state of seizure control,30 we should routinely evaluate depression and suicidality in PWE until future clinical trials with validated instruments determine whether the possible signal observed by the FDA is real.
Sex and age appear to be important factors in predicting suicide. According to a report of the Korean Institute of Criminology, the rate of suicide in Korea is 2.3-fold higher among males than among females, and was highest in the elderly.2 However, we could not substantiate these findings in our PWE cohort; moreover, these factors were not found to be predictors of suicide.
Neurologists are not expected to manage the psychiatric disorders of PWE with suicidal ideation or behavior; however, it should be possible to identify the risks of suicidality from knowledge of the patient's current or past history of mood disorder, family history of mood or suicidal behavior, and previous suicide attempts.31 Self-report instruments aimed at identifying major depressive episodes, such as the BDI17 and the Hospital Anxiety and Depression Scale,32 can be implemented to measure the severity of depressive symptoms. Recently, a simple, six-item self-rating screening instrument, the Neurological Disorders Depression Inventory for Epilepsy, which takes less than 3 minutes to complete, was developed to identify major depressive episodes specifically for PWE.33 A score on this scale of ≥15 is suggestive of a major depressive episode and should be lead to referral to a psychiatrist for further evaluation.
The limitation of our study was that we did not consider psychosocial issues as risk factors for suicide. Among various psychosocial factors, such as family issues, life stress, physical health, previous suicide attempt, and access to firearms,6,11 a history of suicide attempt is the strongest predictor for a successful suicide attempt. For example, PWE who attempted suicide had a 38-fold increased risk of a subsequent successful suicide compared with the general population.34 Likewise, in a Swedish population-based study, a previous suicide attempt was identified in 46% of PWE who eventually committed suicide.7 As a major determinant of suicidality, depression also seems to be correlated with a lack of occupational and social activity, or an unmarried state.35,36 Therefore, further studies should be conducted to establish the impact of psychosocial factors on suicide or depression.
Despite its limitations, to our knowledge this is the first study to clarify the risk factors for suicidality in PWE living in Korea. We established that major risk factors for suicidal ideation in PWE were depressive and psychiatric symptoms, rather than seizure-related variables. Therefore, clinicians should focus on screening for depression and other psychiatric problems and treat them appropriately to prevent PWE from developing suicidal behaviors. Since seizure-related variables also play a minor role in determining depressive symptoms, we should seek stronger risk factors for depression, such as seizure severity or psychosocial factors, to minimize the suicidal behavior.




 XML Download
XML Download