

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
An increase in intrathoracic pressure (ITP) is frequently encountered during many daily straining activities, such as playing wind instruments, coughing, vomiting, lifting heavy loads, and defecation. Its hemodynamic effects have been studied extensively during the Valsalva maneuver.1 Recent studies have suggested that paradoxical embolization through a patent foramen ovale (PFO), caused by elevated ITP, could lead to stroke.2-4 However, very little is known about the effects of raised ITP on the incidence of stroke. We report herein the occurrence of cardioembolic strokes in four young individuals during situations that involved an increase in ITP.
Case Report
Case 1
A 35-year-old male visited the emergency room due to dysarthria and left hemiparesis 30 minutes after the onset of symptoms. These symptoms developed during repeated coughing while eating cold noodles. He denied a previous history of hypertension, diabetes mellitus, or stroke. However, he had a 15 pack/year smoking history and a history of atrial fibrillation. A neurologic examination revealed forced eyeball deviation to the right side and left hemiparesis. Diffusion-weighted images (DWIs) revealed a large infarction in the distribution of the right middle cerebral artery (Fig. 1A). Intravenous recombinant tissue plasminogen activator (rtPA) was infused within 2 hours of symptom onset. Carotid duplex and transcranial Doppler measurements performed 4 hours later were unremarkable. His initial symptoms did not improve, and his overall condition gradually deteriorated. Computed tomography (CT) scans taken 8 hours after the onset of symptoms revealed massive brain swelling with a mass effect and small hemorrhagic transformation. As a result, right-sided hemicraniectomy was performed. The patient regained consciousness 2 weeks later. A neurologic examination at 2 months after symptom onset revealed only mild left-sided hemiparesis.
Case 2
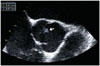
A 24-year-old woman experienced language difficulties and an inability to control her right arm and leg during sexual intercourse. She was a nonsmoker and had no history of hypertension, diabetes mellitus, or previous stroke. Her last menstrual period had occurred more than 1 month prior to the episode, and a positive result in a urine pregnancy test indicated that she was pregnant. The initial neurologic examination revealed left-sided eyeball preponderance, sensory aphasia, and right hemiparesis. DWIs revealed an infarction in the left insular cortex (Fig. 1B). Transthoracic echocardiography revealed an abnormal left-to-right shunt flow through the interatrial septum at rest (Fig. 2). This observation was confirmed to be an atrial septal defect by transesophageal echocardiography. On the following day, the right-sided motor weakness had resolved and sensory aphasia was also partially improved.
Case 3
A 22-year-old woman visited the emergency room due to right-sided paresthesia 30 minutes after onset of the symptoms. These symptoms appeared during severe vomiting on the morning following a night of heavy alcohol drinking. The initial neurologic examination showed right homonymous upper quadrantanopsia, right hypesthesia, and right hemiparesis. MRI revealed two distinct acute infarctions in the left thalamus and occipital lobe (Fig. 1C). CT angiography showed no evidence of extracranial or intracranial dissection. Intravenous rtPA was infused within 3 hours of symptom onset. Gadolinium-enhanced magnetic resonance angiography performed on the third day showed no evidence of atherosclerotic vascular disease or dissection. Transesophageal echocardiography showed a PFO with right-to-left shunting during injection of agitated saline at rest. This patient was treated with anticoagulants and discharged on day 12 with only right homonymous upper quadrantanopsia.
Case 4
A 45-year-old male presented with acute onset of incoherent speech that developed after repeated coughing during meals. He had no known hypertension, diabetes mellitus, or previous stroke. However, he was a current smoker. A neurologic examination showed global aphasia and right-sided facial palsy. DWIs revealed an acute infarction in the distribution of the left middle cerebral artery (Fig. 1D). CT angiography showed no evidence of atherosclerotic vascular disease or dissection. Transesophageal echocardiography showed a small movable mass attached to the aortic valve, which was suspected to be a papillary fibroelastoma on the aortic valve (Fig. 3). This patient was treated with anticoagulants, which improve his global aphasia.
Discussion
All four young patients constituting the present series of cases were found to have a potential cardiac source of embolism. Despite a thorough work-up, no other possible cause of stroke was identified. What distinguishes our study from others is that all of our patients developed signs of stroke at a time when ITP was suddenly elevated by coughing, vomiting, or sexual intercourse.
There are a few reports of ischemic strokes occurring during situations that produced an increase in ITP in patients with PFO, as in our cases 2 and 3 (i.e., while playing a wind instrument or during sexual intercourse).3,4 These reports suggest that the increase in ITP was the probable pathophysiological step that ultimately led to paradoxical embolism. However, right-to-left shunt occurred at rest in our cases 2 and 3, suggesting that while such an increase in ITP is not required to precipitate paradoxical embolization, it can increase the likelihood of such an event. Moreover, the patient in case 2 was predisposed to a prothrombotic state due to her pregnancy. The potential to shunt from right to left in combination with the hypercoagulable state of pregnancy may increase the risk of paradoxical embolism, especially with an increase in ITP.5
Interestingly, two of the patients presented here had a cardioembolic source other than PFO, such as atrial fibrillation and papillary fibroelastoma. In addition, they developed their symptoms during repeated cough. It is possible that the occurrence of the stroke during coughing was a coincidence. However, it is also possible that the stroke was provoked by coughing. In those cases, the pathomechanism is not clear and we can only speculate as to the underlying mechanisms. One possible explanation is that the transient hypoperfusion during an increase in ITP plays a role in the induction of stroke. A case of cough-induced transient hemiplegia was previously described in a patient with contralateral internal carotid artery occlusion and a poor collateral blood supply,6 which led to cerebral hypoperfusion due to increased ITP during repeated cough being proposed as a stroke mechanism. The increase in ITP restricts the venous return and is transmitted via the great veins to the intracranial compartment, causing transient elevated intracranial pressure.1 The resulting reduction in cerebral perfusion pressure can cause an impairment in the cerebral blood flow.1,7 This decrease in cerebral blood flow impedes the clearance of emboli.8 Therefore, in our cases 1 and 4, cerebral ischemia may have been precipitated by a combination of elevated ITP-induced cerebral hypoperfusion and embolization with a reduced washout of emboli.
A change in heart rate during coughing is also a possible explanation. When there is an increase in ITP in response to various situations, including coughing, patients in atrial fibrillation present an increased heart rate. However, unlike normal individuals,1 they do not have the subsequent reflex that normally slows the heart rate as the elevated ITP is relaxed.9 Autonomic modulation of the ventricular rate in patients with atrial fibrillation is less dependent on vagal tone because the sinoatrial node is not functioning properly.10 There is a relative increase in sympathetic tone at the atrioventricular node, which, coupled with a decreased parasympathetic effect on the sinoatrial node,9,10 is thought to be the cause of persistent tachycardia. Therefore, persistent tachycardia due to increased ITP in patients with atrial fibrillation could precipitate embolization, suggesting an additional mechanism of stroke in our case 1.
This study was subject several limitations that should be addressed in order to clarify the putative association between increased ITP and the occurrence of embolic stroke. First, the selection of patients might have been biased, since the occurrence of stroke depended on the clinical history reported by each patient. Second, it is possible that the elevated ITP in our patients as a fortuitous event rather than a pathophysiological condition related to the occurrence of strokes.
In summary, increased ITP due to cough, vomiting, or sexual intercourse may precipitate embolization in patients with PFO, atrial fibrillation, or papillary fibroelastoma. We suggest that cardioembolic stroke is expedited by elevated ITP.


 XML Download
XML Download