

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Occipital neuralgia (ON) is a condition characterized by a paroxysmal stabbing pain in the area of the greater or lesser occipital nerves; clinicians usually regard it as idiopathic.1,2 Some have suggested that ON is the result of trauma or injury of the occipital nerves or their roots; tumor has rarely been reported as a cause.2 We report herein a patient with ON as the only presenting symptom of meningioma in the craniocervical junction in order to alert clinicians to consider the underlying causes of ON.
Case Report
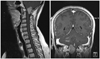
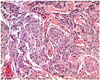
A 55-year-old woman presented with increasing episodes of a paroxysmal headache on the right occipital region, superior and posterior to the ear, over the previous 3 months. She complained of abrupt-onset, sharp, electric-like pain in the right occiput radiating toward the vertex. The pain was triggered by neck flexion or lifting heavy things with both hands. She perceived a dull ache in the right occipital region while lying down on her back. A neurological examination produced normal results with no hypesthesia in the affected area, no cranial autonomic features, and no occipital skin lesions. She felt reduced pain after taking oxcarbazepine. Magnetic resonance image (MRI) of the cervical spine showed a gadolinium-enhanced extraaxial mass within the right aspect of the foramen magnum at the craniocervical junction, measuring 2.7×2.2×2.3 cm (Fig. 1). The mass extended from the medulla oblongata to the C1-C2 level of the spinal cord, deforming the right aspect of the upper cervical spinal cord and medulla and interrupting the right C2 nerve root. The mass was excised and found to be a meningioma that had originated from the arachnoid near the dentate ligament, pushing against the right vertebral artery and encasing the C1, C2, and cranial XI nerves. A microscopy examination confirmed the presence of meningothelial meningioma (Fig. 2). All headaches resolved after surgery.
Discussion
The findings for this patient indicate that a mass in the craniocervical junction can cause ON without other definite neurologic symptoms or signs. It is stated in the literature that most ONs are idiopathic, but that they may arise as a result of inflammation, trauma, or compression of the occipital nerves or their roots, or from an isolated upper cervical cord lesion.2-6 The diagnostic criteria for ON as defined by the International Headache Society (IHS) include paroxysmal stabbing pain with or without persistent aching between paroxysms in the area of distribution of the greater, lesser and/or third occipital nerves, tenderness over the affected nerve, and pain that eases temporarily after local anesthetic nerve block.1 The pain is thought to emanate mainly from the greater and lesser occipital nerves or the nerve roots of C2 or C3, which are the origins of the greater and lesser occipital nerves.1-3 Even though our patient fitted the current IHS criteria for ON except one criterion of a decrease in pain with anesthetic blockade, prolonged pain for as long as 3 months and pain aggravation with head flexion or when lifting heavy objects suggested the presence of a structural lesion. In our case, the initiation of pain that was apparent following head motion and lifting might be attributable to increased pressure inside the cranium causing pressure on the mass, resulting in excruciation of the C2 nerve root. Mass lesions such as osteochondroma, schwannoma, or arthrosis of the C1-C2 joint involving the C2 root have been reported to cause ON without other definite neurological signs.4-6 Common characteristic features of these ON cases with mass lesions are prolongation of the period of ON up to 1 year and pain exacerbated by neck motion. Idiopathic ON cases may present with pain aggravation with neck motion, but this is rare. Therefore, careful medical attention and consideration of cervical spine MRI are needed for ON produced by neck motion that has persisted for a relatively prolonged period.
Meningiomas account for approximately 25% of all spinal tumors; only 2% of spinal meningiomas occur in the foramen magnum.7 Meningioma of the foramen magnum is a potentially lethal condition when unrecognized, resulting in progressive myelopathy with quadriplegia, dysphagia, and sphincter disturbance.7 In our patient, the foramen magnum meningioma deformed the upper cervical cord and medulla; however, it presented with ON as the only symptom without any signs of myelopathy. Because of its rarity as a cause of ON, prompt diagnosis of the compressive lesion is difficult and hence may be delayed. The early diagnosis of compressive lesions in ON is important not only because this offers the possibility of curing the condition, but also because an unrecognized foramen magnum mass is a potentially lethal condition. Careful evaluation of the upper cervical spine and posterior fossa is therefore mandatory, particularly in the setting of ON aggravated by neck motion. The present case broadens the spectrum of causes of ON and suggests that cervical spine MRI is useful in ON even without clinically definite evidence of myelopathy.
 XML Download
XML Download