

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Patients with epilepsy often experience cognitive dysfunction. Antiepileptic drugs (AEDs) can also adversely affect cognitive function by suppressing neuronal excitability or enhancing inhibitory neurotransmission. In general, the effects on cognition are less severe with modern AEDs than with the "classic" AEDs, with the exception of topiramate (TPM) and zonisamide.1-4 Levetiracetam (LEV) is one of the modern AEDs; it has been demonstrated to be effective in the treatment of symptomatic and idiopathic epilepsy,5,6 and has been reported to have no adverse effects on cognition.
A recent randomized, double-blind, crossover study of LEV versus carbamazepine (CBZ) in healthy volunteers revealed better results on half of the neuropsychological measures under LEV, whereas none of the results on the measures were superior under CBZ.7 Two of four adjunctive trials of LEV in patients with refractory partial epilepsy (RPE) reported improved cognitive function,8,9 whereas other studies found no effect.10,11 The mechanisms underlying the improvement in cognitive function by LEV remain unknown. It is thought that it may act by controlling seizures and suppressing epileptiform discharges.12 The pharmacological properties of LEV may include neuroprotective effects against brain insults.13 Thus, it would be useful to elucidate the mechanism of LEV-induced improvements in cognitive function using electrophysiology studies and/or neuroimaging.
Electroencephalogram (EEG) studies of neurocognitive function have focused on the frequency band over 20 Hz. It has been shown in human EEG studies that the cortical high-frequency activity is topically enhanced in various cognitive processes.14-17 Complex cognitive tasks ignite neuronal cell assemblies and activate loops of neuronal network. In the case of the language process, a loop between Broca's region and Wernicke's region is activated.18 The neuronal oscillation is equivalent to a circulation frequency of 25-30 Hz. In contrast, higher-frequency oscillatory cortical activity, in the range 40-60 Hz, is seen in less widely dispersed cell assemblies.19 The increase in gamma power synchronization of evoked gamma activity may indicate a general mechanism that enables transient associations between neuronal assemblies. The synchronized gamma activity also may be relevant to selective attention.20
It is difficult to establish the brain current source by visual inspection of multichannel EEG data, because many combinations of current sources with various locations and strengths in the brain may generate signals in the scalp electrodes. Current-source analysis (CSA) using digital EEG data can be used to directly measure neuronal activity. CSA uses mathematical methods to analyze the electrical potentials on the scalp electrodes and to determine the exact location of current sources.21
Low-resolution brain electromagnetic tomography (LORETA) is a method of CSA that utilizes a distributed-current-source model. This discrete and linear solution computes a unique 3-D electrical source distribution by assuming that the smoothest of all possible inverse solutions is the most plausible, and is consistent with the assumption that neighboring neurons are active simultaneously and synchronously. The technique localizes the current source of cerebral activity by current density reconstruction and makes it possible to obtain 3-D functional images.22 This study investigated changes in the brain current-source density (CSD) in the high beta frequency band (22-30 Hz) induced by LEV adjunctive therapy in patients with RPE. We compared these changes with the seizure frequency and the LEV dosage in these patients.
Methods
Subjects
RPE patients were recruited from those attending our epilepsy clinics. Enrollment was limited to adult patients (aged 19-60 years) whose partial-onset seizures (simple or complex partial with or without secondary generalization, according to the International League Against Epilepsy classification) were poorly controlled by AEDs. Our definition of RPE was partial epilepsy that is uncontrolled by two or more AEDs and having a frequency of at least once per month over 6 months before entry into the study. We included only right-handed persons to exclude the effects of handedness on the cerebral current-source distribution. Patients with progressive neurological disorders, head injury, mental retardation (IQ<70), alcohol or drug abuse, ongoing use of any centrally acting medications, severe psychiatric problems, or other severe medical disorders were excluded. We acquired demographic and epilepsy-related characteristics through an epilepsy questionnaire and the patients' diaries.
Study design
A cohort of 31 RPE patients was enrolled in a 24-week, open-label, prospective study. Before prescribing LEV, all patients gave their written informed consent to participate in the study. We added LEV to each patient's current AED regimen. The study included a baseline phase of 12 weeks and then a 4-week interval of titration of LEV (250 mg twice daily in the first 2 weeks, 500 mg twice daily in the 3rd and 4th weeks); thereafter, the dose regimens were adjusted individually based on the investigator's clinical judgment according to the patient's clinical response and tolerability, to obtain the best seizure control and tolerability. The LEV dosage was titrated up to 3,000 mg/day if the attacks had not subsided. Seizure frequency and scalp EEG were recorded, and neuropsychological tests (NPTs) were conducted before the LEV trial and after 24 weeks of therapy. Mood tests were conducted to clarify the effect of mood on cognitive performance. EEG recordings and NPTs were conducted on the same day.
We observed LEV-induced CSD changes and determined whether there was any association between these changes and the presence of freedom from seizure or dosage of LEV. For the comparisons, we subdivided patients into the following two groups: 1) patients with seizure freedom versus those who were not seizure-free, and 2) patients taking at least 2,000 mg/day LEV versus those taking less than 2,000 mg/day LEV. We also compared the results of NPTs conducted at 24 weeks with those conducted at baseline.
EEG recording
EEGs were recorded for at least 30 min in each patient using a 32-channel digital EEG machine (Telefactor Aurora® EEG machine, Grass-Telefactor, Melbourne, Australia). All EEGs were recorded at 200 Hz using 19 channels based on the international 10-20 system (Fp1, Fp2, F3, F4, C3, C4, P3, P4, O1, O2, F7, F8, T3, T4, T5, T6, Fz, Cz, and Pz).
Current-source analysis by cross-spectral analysis using low-resolution brain electromagnetic tomography
After recomputing to the average referential montage, five 3-s, artifact-free segments were selected from the recording of each EEG (filtered from 1.6 to 70 Hz) from segments of the waking state with no epileptiform discharge. We used the data review and processing module in the Brain Electrical Source Analysis software (v. 5.1, MEGIS, Grafelfing, Germany) to obtain the segments. Frequency-domain analysis in the 22-30 Hz frequency band was applied to the selected 3-s artifact-free segments (600 sample points). LORETA-KEY (KEY Institute for Brain-Mind Research, Switzerland) was used to calculate the intracerebral current density in the frequency-domain analysis.
Our version of LORETA used a three-shell spherical head model, registered to the Talairach human brain atlas, and the data available as digitized magnetic resonance images from the Brain Imaging Center of the Montreal Neurologic Institute.23 The registration between the spherical and Talairach head geometries used the realistic EEG electrode coordinates reported by Towle et al.24
Neuropsychological tests
All NPTs were conducted in a sound-attenuated, temperature-controlled room by a single examiner. According to the literature and our own clinical experience, several cognitive measures were selected as being particularly sensitive in epilepsy patients. The following parameters were assessed:
1) Memory function using list learning (LL), immediate and delayed word recall (IWR and DWR), word recognition, and visual reproduction based on the Memory Assessment Scale obtained from Psychological Assessment Resources.26
2) Attention deficit using forward and backward digit spans from the Wechsler Memory Scale-Revised.27
3) Attention, visuomotor tracking abilities, and mental flexibility with the Trail-Making Test, Parts A and B (TMTA and TMTB, respectively) from the Halstead-Reitan Battery.28
4) Verbal fluency using semantic fluency tests from the Boston Diagnostic Aphasia Examination, Third Edition.29
Statistical analysis
Five segments of 3-s epochs were selected from a test EEG and a retest EEG from each patient. Thus, a total of 120 EEG data pairs (24 patients×5 epochs×2 conditions) were obtained. Paired sample t-tests were computed for the log-transformed LORETA power at each voxel in the 22-30 Hz frequency band to evaluate differences between the two conditions. In all analyses, the level of statistical significance was set at p<0.05. These voxel-by-voxel t values were displayed as statistical nonparametric maps (SnPMs).
For the NPTs, higher scores indicated better performance in all cognitive tests, except the TMTA and TMTB, for which higher scores indicated worse performance because the time required was defined as the dependent measure for these tests. Data for continuous variables are expressed as mean±SD values, and data for categorized variables are expressed as frequencies (percentages). The paired t-test was used to evaluate the test-retest changes in neuropsychological scores induced by LEV adjunctive therapy. The statistical analyses were conducted with SPSS 12.0 (SPSS, Chicago, IL, USA), and results were deemed to be statistically significant at p<0.05.
Results
Patients
Four of the 31 enrolled patients dropped out during the titration period due to central-nervous-system-related side effects or rash. One patient stopped using LEV due to aggravation of seizures. Two patients were excluded due to unsuitable EEG data. A total of 24 patients completed follow-up EEGs and NPTs. Their demographic and clinical characteristics are summarized in Table 1. After 24 weeks of treatment, the frequency of seizures was significantly decreased (p<0.05). The response rate was 54%, and seizure freedom occurred in 33% of the patients at a mean LEV dosage of 2,260 mg/day. The incidence of adverse events in the last 4 weeks was 29%. The most common adverse events were somnolence and asthenia. The findings of brain magnetic resonance imaging (MRI) were normal in 17 of 24 patients, with the remaining 7 patients showing the following abnormal MRI findings: right frontal schizencephaly, left frontal traumatic contusion, left hippocampal sclerosis, left hippocampal sclerosis with temporal arachnoid cyst, both temporal encephalitis, left temporoparietal arachnoid cyst, and left occipital hypoxia.
Current-source analysis
The CSD in the 22-30 Hz frequency band was increased in the bilateral anterior cingulate gyri, left parahippocampal gyrus, and a small area of the right anterior parahippocampal gyrus after the LEV trial (p<0.05)(Fig. 1). The CSD in a small area of the bilateral superior parietal gyri was higher in patients who were free of seizures (n=8) than in those who were not seizure-free (n=16, p<0.05)(Fig. 2A). The CSD in a small area of the bilateral precunei was lower in patients taking at least 2,000 mg/day LEV (n=15) than in those taking less than 2,000 mg/day LEV (n=9, p<0.05)(Fig. 2B).
Neuropsychological tests
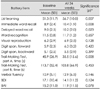
The result of NPTs and mood tests before and after the LEV trial are summarized in Table 2. Performances in verbal memory tests, such as LL, IWR, and DWR, were significantly improved after the 24-week LEV trial (p=0.007, 0.008, and 0.023, respectively). Executive function, such as TMTA, was also improved at the follow-up test (p=0.008). There was no deterioration on any of the tests. Mood states were not significantly changed at 24 weeks.
Discussion
To our knowledge, this is the first study to examine the changes in current source induced by LEV adjunctive therapy in RPE patients. The CSD in the high beta frequency band was increased in the bilateral anterior cingulate gyri, left parahippocampal gyrus, and a small area of the right anterior parahippocampal gyrus after the LEV trial. Neither seizure freedom nor the dosage increment of LEV elicited meaningful CSD changes. We demonstrated that verbal memory and executive functions had significantly improved after 24 weeks of the LEV trial. Thus, we suggest that LEV enhances the activities of the neuronal networks in the prefrontal cortex and left hippocampus.
Previous studies on experimental animals and epileptic patients have shown that LEV does not impair cognitive function.8,32 In addition, it was suggested that LEV administration improves neurocognitive function and quality of life in epileptic patients.7-9,33,34 LEV is a derivative of piracetam and is a pyrroline-type compound. Piracetam improves learning, memory, and attention.35 Drugs in this class exert protective effects against brain insults,36 promote the efficacy of the higher integration mechanisms in the brain, and improve mental functions such as learning and memory.37 Our patients with RPE showed improved cognitive performance after 24 weeks of LEV administration. These findings are consistent with those of Piazzini et al.8 and Zhou et al.9
Digital EEG analyses of the neurocognitive effects of epilepsy and AEDs have been conducted previously. We found three studies that sought to correlate digital EEG analyses with the neurocognitive effects of AEDs drugs in healthy volunteers.38-40 In one study, both CBZ and gabapentin (GBP) were shown to reduce the peak frequency of the posterior alpha rhythm, with the change being larger for CBZ than for GBP. Among the NPTs, the digital symbol test and Stroop test were affected by AEDs.38 In another study, both oxcarbazepine (OXC) and phenytoin slowed the EEG peak frequency and increased the relative theta and delta powers. Significant cognitive effects primarily appeared in measures of motor speed and reaction time for both AEDs. The only significant difference between AEDs was for mood, favoring OXC.39 In another study, TPM produced no significant change in any EEG measure from the averaged occipital electrodes, although several target NPTs revealed negative effects of TPM. However, GBP slowed the peak and median frequency EEG measures and increased the percentage of theta and delta activities.40
Another study with a very similar design to ours41 analyzed the occipital EEG rhythms using the fast Fourier transform in 28 patients with pharmacoresistant epilepsy. LEV adjunctive therapy did not slow EEG rhythms over the occipital regions at 2 months after the initiation of therapy and achieving the end-dose, or at 4 months after achieving plateau dosing as compared with baseline measures. In other words, there were no changes in alpha, theta, and delta bands. In addition, the percentage of activity in the beta band increased. Our study used the distributed source model of CSA, which has not previously been applied to test the cognitive effects of AEDs.
Task-related high-frequency oscillations include two functionally distinctive components. Complex cognitive tasks, such as language processing, are associated with neuronal oscillation at frequencies of 25-35 Hz.18 In a study using EEG and magnetoencephalogram experiments, spectral responses of about 30 Hz were specifically induced by a language process using meaningful words but not by meaningless nonwords.15 In contrast, the processing of simple stimuli affects the spectral power in the higher-frequency range of the gamma band. Tones, moving bars, and simple repetitive movements are usually accompanied by spectral activity at 40 Hz or above.19 The increase in high-frequency synchronization may indicate a general mechanism enabling transient associations between neuronal assemblies.
Regarding our results, the CSD in the high beta frequency band was increased in anatomical structures relevant to the improvement in NPTs. Since the left hippocampus is functionally important for verbal memory, the increase in CSD in the left parahippocampal gyrus may reflect the improvement in verbal memory function. The cingulate gyrus is a part of the prefrontal cortex, which is functionally important for executive tasks, and so the increase in CSD in the bilateral anterior cingulated gyri suggests improved executive function.42 Neither seizure freedom nor the dosage increment of LEV elicited meaningful CSD changes. The changes in CSD suggest a stimulatory effect of LEV on cognition.
The present study has some limitations. We used fewer than the 32 available channels, which could have resulted in some localization errors, particularly in the basal aspects of the brain.43 The localization accuracy for LORETA has been shown to increase when using from 25 to around 89 electrodes, and then to plateau thereafter.44 However, a lower number of electrodes may be sufficient for the SnPM method of LORETA to localize the areas of increased activity.45,46 It has also been observed that current-source estimation using LORETA in a three-shell head model is similar when using between 19 and 46 scalp electrodes when the electrodes are evenly distributed.44 Our version of LORETA used a three-shell spherical head model instead of a realistic head model. The errors associated with using a spherical model with a small number of electrodes range from 10 to 20 mm.43,47,48 Using a greater number of more closely spaced electrodes would have enhanced the topographical resolution and produced better current-source localization results.
There were also several limitations with regard to the NPTs. First, the sample of patients was relatively small. Second, because this was not a randomized, placebo-controlled study, we cannot exclude a placebo effect of LEV on cognition. Third, because LEV was added to other AED regimes, we cannot rule out the impact of other AEDs on cognition. Further cognitive studies of LEV based on blind or placebo-controlled, monotherapy trials with larger numbers of patients are needed to obtain clearer and more reliable answers to these issues.



 XML Download
XML Download