

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute encephalopathy can result from various causes, including stroke, seizure, metabolic disturbance, toxic material, and infection.1-4 Hashimoto's encephalopathy (HE) is also one of the causes of treatable encephalopathy. Since the first report of Brain et al.,1 there have been more than 100 patients reported with HE, which has also been termed steroid-responsive encephalopathy with autoimmune thyroiditis (SREAT) in a recent report.2,5 HE or SREAT is known to be associated with autoimmune thyroid disease (AITD). However, to our knowledge steroid-responsive encephalopathy associated with subacute thyroiditis has never been reported. Here we report a case of steroid-responsive recurrent encephalopathy that manifested simultaneously with subacute thyroiditis.
Case Report
A 49-year-old woman was brought to our institution due to decreased mentality, dysarthria, and gait disturbance. She had been found collapsed and confused in her bedroom by her daughter. She had experienced an upper respiratory infection 4 weeks before admission, and had also suffered from hypertension. Her highest level of education was elementary school and she was right-handed. On admission her temperature was 37.6℃ and pulse rate was 93 beat/minute. She had mild goiter, of approximately 25 g, and thyroid tenderness. The neurologic examination revealed somnolence, memory impairment, dysarthria, right-hand weakness, and gait disturbance. The initial impression was acute stroke or seizure.
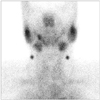
However, the results of brain magnetic resonance imaging (MRI) including diffusion-weighted imaging and angiography were normal. Electroencephalography revealed only intermittent generalized delta slowing without epileptiform discharges. Her serum levels of total T3, free T4, and thyroid-stimulating hormone (TSH) were 392 ng/dL (reference range: 80-180 ng/dL), 2.82 ng/dL (reference range: 0.8-1.8 ng/dL), and <0.01 mU/L (reference range: 0.3-5.0 mU/L), respectively. The serum and cerebrospinal fluid (CSF) were negative for both antithyroglobulin antibody and antimicrosomal antibody, and TSH-binding inhibiting immunoglobulin was at 5% (reference range:-10% to 10%). The erythrocyte sedimentation rate was 101 mm/h. Thyroid ultrasound revealed a mildly enlarged thyroid and heterogeneous hypoechogenicity with a lobulating contour in both thyroids. A thyroid scan showed a markedly decreased uptake of 99mtechnetium-pertechnetate (Fig. 1), and fine-needle-aspiration cytology revealed multinucleated giant cells in the background of inflammatory cells (Fig. 2). These findings were compatible with the thyrotoxic phase of subacute thyroiditis. The CSF examination was normal except for positivity for 14-3-3 proteins. Venereal Disease Research Labo (VDRL) was nonreactive and lupus erythematosus (LE) cells were not found. Paraneoplastic antibodies were negative. Antineutrophil cytoplasmic antibodies (ANCA), antiphospholipid antibody, anticardiolipin antibody, lupus anticoagulant, antinuclear antibody, anti-dsDNA, anti-Sm, anti-RNP, anti-Ro, anti-La, anti-Scl-70, anti-Jo-1, and anti-SS-Ro52 were all within normal limits. Single-photon-emission computed tomography demonstrated no perfusion abnormality.
On the second day of admission, the patient became more somnolent and exhibited dysmetria on the right side. She was given a nonselective beta-blocker (propranolol), but there was no clinical improvement during the following 5 days. The score on the Korean Mini Mental Status Examination (KMMSE) was 21/30 on the fifth day of admission. On the sixth day of admission she was started on oral prednisolone (30 mg/day) in addition to the propranolol for 7 days. Her mental status began to improve from the next day. Five days after beginning steroid treatment, she could walk with assistance, at which time a thyroid function test (TFT) indicated that her serum levels of total T3, free T4, and TSH were 128 ng/dL, 0.93 ng/dL, and <0.01 mU/L, respectively. The gait disturbance, dysmetria, and somnolence gradually improved thereafter, with the K-MMSE score improving to 25/30. She was discharged on an antiepileptic drug. One month later she could walk without assistance and showed only mild dysarthria.
Two months after the initial admission, she felt numbness on the right side. It became difficult for her daughter to understand her speech and she could not walk without assistance. However, there was no clinical or laboratory evidence of recurrent viral infection. A repeated TFT demonstrated hypothyroidism, with serum total T3 at 42 ng/dL, free T4 at 0.59 ng/dL, and TSH at 73.9 mU/L. These changes in TFT results were attributed to the typical natural course of subacute thyroiditis, and 50 µg of thyroxine replacement was initiated and then gradually increased to 100 µg. Four weeks later, TFT results showed improvement of hypothyroidism, with serum total T3 at 85 ng/dL, free T4 at 0.74 ng/dL, and TSH at 43.0 mU/L. However, her symptoms persisted. A repeated brain MRI produced normal results. Steroid pulse therapy (methylprednisolone, 1 g/day) was given for 3 days, after which oral prednisolone was prescribed. She began to improve from the next day of steroid pulse therapy. Two weeks later, gait disturbance and dysarthria were improved and she complained of only mild numbness on the right side.
Discussion
To our knowledge this is the first reported case of steroid-responsive recurrent encephalopathy associated with subacute thyroiditis, which was diagnosed by thyroid tenderness, markedly decreased uptake of 99mtechnetium-pertechnetate on the thyroid scan, and thyrotoxicosis followed by hypothyroidism on TFT. Encephalopathy was improved with steroid treatment. After we excluded vascular, toxic, metabolic, and infectious disease, our patient was tentatively diagnosed as steroid-responsive recurrent encephalopathy of unknown cause. It was very interesting that the clinical manifestations were similar to those of HE. However, there was no evidence of AITD.
Various clinical manifestations of HE or SREAT have been reported.2,5-11 Cognitive impairment, high serum concentrations of thyroid autoantibodies, and good responsiveness to steroid treatment have been described as common clinical features and accepted as diagnostic criteria of HE or SREAT.1,2,5-9,12,13 However, it is questionable that AITD is necessary in the diagnosis of HE or SREAT since there is no conclusive evidence that this encephalopathy is caused by Hashimoto's thyroiditis or other autoimmune thyroiditis.2
AITD is prevalent in the general population,6 and there are no consistent correlations between the clinical severity and the type of thyroid antibody, or the clinical severity and the serum concentration of thyroid autoantibodies.2,5,6,9,12 It has been suggested that thyroid autoantibodies are not the cause of encephalopathy, but rather simply a marker of some autoimmunity affecting the brain, such as humoral immunity by antineuronal antibody as detected in one patient with HE.5,11 Therefore, it appears unreasonable to assume that thyroid autoantibodies are required for a diagnosis of HE. The clinical manifestations of our case were similar with those of HE except for the absence of thyroid autoantibodies.2,5,6 Considering that thyroid autoantibodies have played no pathogenic role in patients with HE and that HE is a syndrome entity rather than a disease, we tentatively diagnosed our patient as HE without AITD. However, tests for the definitive diagnosis of HE do not exist, and hence our hypothesis could not be verified in this single case. More observations are needed to examine this hypothesis.
Our case showed dramatic neurological improvements following steroid treatment, which is one of the typical clinical characteristics of HE.2,5,6,9-12 Despite considerable debate about whether steroid responsiveness can be used in the diagnostic criteria of HE,2,5 a beneficial response to a steroid might be the only evidence of autoimmunity6 or the only feature differentiating HE from Creutzfeldt-Jakob disease, especially in patients with 14-3-3 proteins in the CSF.14,15
The 14-3-3 proteins comprise about 1% of total soluble protein in brain16 and are known to be involved in certain neurological disorders such as Creutzfeldt-Jakob disease, HE, influenza-associated encephalopathy, and steroid-responsive encephalopathy.7,15-17 Examination of the CSF in our case revealed positivity for 14-3-3 proteins, which suggested that the encephalopathy was not associated with a functional disorder, but rather with neuronal damage in the brain.17 Considering the responsiveness to steroid treatment, steroid should be given as soon as possible to patients with suspected HE since delaying treatment might lead to irreversible brain deficits.
There has been considerable debate about whether thyroid dysfunction can cause encephalopathy in patients with HE.5,7,9,11,12 Although there is one report of thyrotoxicosis preceding clinical relapse of encephalopathy, antithyroid medication did not improve neurologic deficits and variable thyroid functions including hyperthyroidism, hypothyroidism, and euthyroidism in patients with HE.5,7,9 However, to our knowledge there has been no report of encephalopathy associated with both thyrotoxicosis and hypothyroidism.
Subacute thyroiditis occurred simultaneously with encephalopathy in our case, and the encephalopathy was unlikely to have been caused by the thyroid dysfunction induced by subacute thyroiditis since the encephalopathy occurred both in the thyrotoxic and hypothyroid states. Furthermore, the neurologic deficits were not improved for management of thyrotoxicosis during the thyrotoxic phase and thyroid hormone replacement during the hypothyroid phase of subacute thyroiditis. On the contrary, steroid treatment induced marked improvement of neurologic deficits. Our observation was compatible with thyroid dysfunction not being the cause of neurologic deficits, and hence another mechanism might have played a role in the pathogenesis of encephalopathy. A common underlying pathomechanism such as common autoantibody to thyroid and brain is another possible explanation of our case, although we did not detect any abnormal autoantibody levels in the patient's serum.11 To the best of our knowledge, this is the first case report of steroid-responsive encephalopathy associated with subacute thyroiditis.
In conclusion, steroid-responsive encephalopathy associated with subacute thyroiditis might be a subtype of HE. Steroid treatment should not be delayed in suspected patients since the encephalopathy is associated with neuronal damage.

 XML Download
XML Download