

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cerebral fat embolism is an uncommon but serious complication of long-bone fractures. Although such embolisms are diagnosed on the basis of clinical manifestations accompanied by hypoxemia, neurologic dysfunction, and petechiae, their neurologic symptoms are variable and often nonspecific. There are several reports of magnetic resonance imaging (MRI) being a useful diagnostic tool for assessing cerebral fat embolism,1,2 with a few reports emphasizing that abnormal findings on diffusion-weighted MRI (DWI) have significant diagnostic value in acute cerebral fat embolism.3,4 The pathogenesis of disruption of the blood-brain barrier by cerebral fat embolism is still unclear, but it is thought that fat globules occlude the microvasculature, producing necrosis and hemorrhage in the surrounding parenchyma.5 Local inflammatory and toxic reactions by free fatty acid causes breakdown of the blood-brain barrier.6 Considering that the pathologic findings in cerebral fat embolism are characterized by multiple petechiae and purpura, and that T2*-weighted gradient-echo MRI is a sensitive method for detecting residual hemorrhage, this MRI sequence might aid the diagnosis of cerebral fat embolism.
To the best of our knowledge, no previous study has emphasized the diagnostic usefulness of gradient-echo MRI in patients with cerebral fat embolism. This report presents a patient with cerebral fat embolism documented by the presence of multiple low signals on T2*-weighted gradient-echo MRI, in whom there was marked resolution of the previous abnormal findings.
Case Report
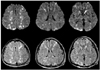
A 54-year-old male suffered from bilateral femoral fractures due to a traffic accident. He was alert and well oriented on admission, but became stuporous with extensor posturing 36 hours after the accident. The findings of basic blood tests, including arterial blood gas, were normal, and the findings of chest X-rays were also unremarkable. Brain computer tomography (CT) performed 3 hours after the deterioration showed normal findings. MRI was performed 10 hours later, with DWI, T2-weighted imaging (T2WI), and fluid-attenuated inversion recovery (FLAIR) images showing multiple high-signal lesions in the bilateral hemisphere.
Multiple lesions were prominent in the subcortical and deep white matter. Other lesions were observed in the thalamus, basal ganglia, corpus callosum, and occipital cortex (Fig. 1). Electrocardiography and echocardiography showed normal findings. Three days later, multiple petechiae were detected on the skin of the anterior chest.
The patient received supportive therapy, and his condition improved slowly. Neuropsychologic testing was not possible due to poor cooperation from the patient. His severe cognitive impairment, which included disorientation, apraxia, acalculia, and memory impairment, lasted for 2 months. Follow-up MRI performed 50 days after the onset of the cognitive impairment showed marked resolution of previous abnormal high-signal lesions and a few subtle remaining white-matter lesions (Fig. 2). In addition, T2*-weighted gradient-echo MRI revealed multiple tiny low-signal lesions distributed over the areas where the previous abnormal lesions had been located.
Discussion
Fat embolism syndrome has nonspecific and variable cerebral manifestations, including headache, lethargy, irritability, convulsions, and coma. Despite the marked neurologic dysfunction in our patient, there were no obvious pulmonary symptoms or signs. There are several reports of isolated neurologic disorder occurring after cerebral fat embolism.7 The history of traumatic bone fractures, delayed onset of a nonfocal neurologic dysfunction, the appearance of petechiae over the anterior chest, and marked abnormal signals over conspicuous sites on MRI supported the diagnosis of cerebral fat embolism in this patient.
Small, scattered, hyperintense lesions on T2WI and FLAIR imaging have been found previously.2-4 These lesions typically appear in the periventricular, subcortical, and deep white matter, as well as in the deep gray matter, including the corpus callosum.8-10 The lesions are usually not detected by CT and are more prominent on DWI than T2WI and FLAIR images, especially during the acute stage. These abnormalities in the signal intensity on DWI presumably reflect the foci of cytotoxic edema. Clinical studies by Simon et al. and Butteriss et al. suggested that focal parenchymal hemorrhage is not a predominant feature in T2*-weighted gradient-echo MRI.8,9 However, their cases might not accurately reflect the full spectrum of patients with cerebral fat embolism because they showed relatively good clinical improvement. The number of white-matter lesions on MRI is correlated with the patient's score on the Glasgow Coma Scale.10 Simon et al. considered that gradient-echo imaging might be useful in determining the severity of cerebral fat embolism, although hemorrhage was not a predominant feature of the multiple white-matter lesions in their reported case.9 Neuropsychological testing has revealed obvious cognitive deficits in patients with stenosis of the internal carotid artery and lesions on the periventricular, subcortical, and deep white matter.11 Periventricular and subcortical white-matter lesions have been associated with worse performance on all cognitive measures tested.12 The patient in the present study exhibited continuous neurologic impairment, and T2*-weighted gradient-echo MRI showed that the lesions were distributed throughout the white matter of the cerebrum.
Reports of serial MRI and gradient-echo MRI in cases of cerebral fat embolism are rare. Previous studies of this condition found improvement of the neurologic impairment and the gradually disappearance of lesions on MRI within a few weeks to a few months. These findings might reflect immediate cytotoxic edema secondary to ischemia and subsequent vasogenic edema developing at a later stage.4 The patient in the present study presented with persistent cognitive impairment during the follow-up period. Follow-up MRI (T2WI and FLAIR) showed that some lesions disappeared, with only subtle ill-defined signal changes remaining. These findings did not explain the persistent neurologic impairment. A T2*-weighted gradient-echo MRI sequence is sensitive to hemosiderin deposits in the brain parenchyma and is very useful for assessing the presence of old and new hemorrhage.13,14 Gradient-echo MRI sequences were not obtained during the initial MRI examination in this patient. However, T2*-weighted gradient-echo MRI in the subacute and chronic stages of the follow-up MRI study in this patient revealed prominent multiple low signals, which might explain the residual neurologic impairment.
The findings of the present study suggest that T2*-weighted gradient-echo MRI can be used to analyze the neurologic impairment in patients with cerebral fat embolism, with the findings also closely reflecting the clinical severity. Gradient-echo imaging is useful for detecting the petechial hemorrhage that is the characteristic pathologic finding of cerebral fat embolism. Gradient-echo MRI might be useful in defining the clinical severity of cerebral fat embolism with diffuse petechial lesions in the subacute or chronic stage, especially when abnormal signals are not detected in other forms of MRI.
In conclusion, MRI can be used for the early diagnosis of cerebral fat embolism with high sensitivity. We suggest that T2*-weighted gradient-echo MRI provides useful information for determining the clinical severity of patients with cerebral fat embolism.

 XML Download
XML Download