

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several epidemiological1-4 and neuroimaging5-7 studies performed during the last 10have provided evidence supporting the vascular pathogenesis of Alzheimer's disease (AD). These studies have suggested that vascular risk factors directly reduce cerebral perfusion to a critical level of dysfunction, enhancing neuronal death in AD.8,9 A recent population-based study using transcranial Doppler sonography (TCD) strongly supports this hypothesis by demonstrating that cerebral hypoperfusion precedes and possibly contributes to the onset of clinical dementia.10 Another study has suggested that cerebral vasomotor reactivity (VMR) is a significant predictor of cognitive decline in AD patients.11
VMR refers to the capability to dilate or constrict cerebral arterioles in response to metabolic stimuli, such as CO2 or acetazolamide, which may be decreased in large-vessel occlusive disease or small-vessel microangiopathy.12 However, VMR has rarely been studied in AD patients, and it has not been clarified whether VMR is lower in AD patients than in nondemented subjects. Using a TCD rebreathing method, we investigated differences in VMR between AD patients and control subjects, which may be related to the vascular pathogenesis of AD.
SUBJECTS AND METHODS
1. Subject inclusion and study design
Dementia patients aged from 55 to 80 years who met the NINDS-ADRDA criteria for AD were included in this study.13 Age- and sex-matched control subjects without dementia were chosen from those who had visited the neurology clinic or health promotion center in Seoul National University Boramae Hospital. The Mini-Mental State Examination (MMSE), MRI, and MRA were applied to all subjects. Subjects who showed territorial infarcts, multiple lacunes, stenosis of the middle cerebral artery (MCA), or bilateral suboptimal temporal window were excluded. Because VMR can be affected by certain drugs such as statins14 and angiotensin-converting enzyme inhibitors,15 those using such drugs were also excluded. All subjects gave their informed consent.
Changes in white-matter lesion severity in MRI were quantified used the Rotterdam Scan Study (RSS) scale,16 which separately scores the periventricular regions (periventricular score range: 0 to 9) and the volume of subcortical white-matter lesions (subcortical score range: 0 to 29.5 mL).
2. TCD assessment and measurement of VMR
With the subject in a supine position, the TCD probe was used in a fixed position to monitor the mean flow velocity (MFV) in the MCA. A rebreathing method was adopted for elevating the CO2 concentration. A 6-L rebreathing bag with several pores was applied to patients via a facial mask for at least 5 minutes, and the CO2 concentration was continuously monitored with a capnometer. Subjects with inadequate CO2 retention (≤ 45 mmHg) were excluded from the analysis. Baseline blood pressure, bilateral MFV, and pulsatility index (PI) were obtained, and MFV was continuously monitored and digitally recorded for later off-line analysis. VMR was calculated as the percentage change in the MFV according to VMR = (MFVhypercapnia-MFVnormocapnia)100/MFVnormocapnia). Validation of this method and normal reference values have been presented previously.17
3. Statistical analysis
Student's t-test was used for intergroup comparisons of continuous values, and the chi-square test was used for comparisons of categorical variables. The correlations of VMR with the MMSE score and the grade of white-matter lesions were analyzed by bivariate correlation analysis. A probability value of p<0.05 was considered significant. All data are presented as mean±SD values.
RESULTS
Seventeen AD patients and 17 control subjects were recruited (age 67.1±5.9 years, range 55 to 78 years; 7 males and 10 females per group). The MMSE score was significantly lower in AD patients than the control subjects (22.1±4.9 vs. 28.7±0.6, p=0.042). Other baseline characteristics - including cerebrovascular risk factors, medications, and grades of white-matter lesions - did not differ significantly between the two groups, as summarized in Table 1.
Four and one AD patients showed suboptimal temporal windows on the right and left sides, respectively. Therefore, we also excluded the corresponding TCD values of the matched control subjects from the analysis. The baseline MFV and PI also did not differ between the AD patients and the control subjects. However, VMR was significantly decreased in AD patients in both the right- and left-side MCAs (Fig. 1): 57.7±22.2 and 36.8±26.0 in control subjects and AD patients, respectively, on the right side (p=0.037); and 58.7±21.1 and 37.2±22.7 on the left side (p=0.014). VMR was linearly correlated on the right and left sides (Pearson's correlation coefficient=0.883, p=0.001).
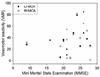
VMR and MMSE scores of AD patients were not significantly correlated either in the right-side (Pearson's correlation coefficient=0.264, p=0.324) or left-side (Pearson's correlation coefficient=0.095, p=0.758) MCA (Fig. 2). VMR of AD patients was not correlated with either the volume of subcortical white-matter lesions or the grade of periventricular white-matter lesions (all p>0.05).
DISCUSSION
Whether AD is a pure neurodegenerative disorder or has contributions from vascular disease remains controversial. In the present study, VMR was lower in patients with mild-to-moderate AD than in age- and sex-matched control subjects. Several TCD studies have shown that the blood flow velocity is decreased in AD,18,19 and one study found an association between VMR and future cognitive decline in AD.11 However, the present report is the first to compare VMR between AD patients and nondemented subjects.
In the RSS study, VMR was reduced in subjects with cognitive decline but not in patients with clinical dementia.10 In addition, the cerebral blood MFV was correlated with both the cognitive decline and the clinical dementia severity.10 However, that study involved only 13 AD patients among 1730 subjects, which might have resulted in a lack of statistical power, and it was suggested that reduced VMR in AD was related to significant vascular comorbidity.10 It has recently been reported that reduced cerebrovascular reactivity predicts cognitive decline in AD patients.11 However, that report presented no information on the level of VMR in the AD patients, and hence on whether VMR decreased with the disease progression.11
In the present study, VMR but not the blood flow velocity was lower in AD patients than in the controls. This suggests that the pathologic changes of AD are more closely related to VMR than to the flow velocity itself. It is known that a reduced VMR is correlated with the severity of microangiopathy, which increases vascular resistance.20,21 In addition, reduced VMR is representative of a reduced vasomotor reserve, which is prominent in hemodynamically significant stenosis or occlusion of the internal carotid artery.10,20 Because cerebrovascular CO2 reactivity is influenced by atherosclerosis through disturbance of the integrity and function of the arterial wall, a reduction in VMR to hypercapnia is indicative of cerebral small-vessel pathology.10,20
Nevertheless, whether reduced VMR is correlated with decreased cerebral perfusion is not yet certain. Critical threshold cerebral hypoperfusion may result in changes to the capillaries, including basement membrane thickening, endothelial cell compression, degeneration of pericytes, and lumen distortion.9 These changes can reduce the capacity of the arterioles to dilate in response to CO2 stimuli, which represents VMR. Consequently, reduced VMR is likely to be related to (or at least associated with) critical hypoperfusion. Direct measurement of cerebral perfusion and metabolism using SPECT or PET will provide more information about the significance of a reduced VMR.
It remains unclear whether the decreased perfusion reflects the diminished demand caused by advanced neurodegeneration, or whether cerebral hypoperfusion precedes and contributes to dementia and neurodegeneration. The decreased delivery of oxygen due to the decreased cerebrovascular reserve can lead to hypoxia in vulnerable areas of the brain, such as watershed areas and the hippocampus,10 and can negatively affect cognitive function. In addition, any events that reduce cerebral blood flow and perfusion can trigger cerebral injury in patients with a reduced VMR.
We found no correlation between the MMSE score and VMR in the present study. In addition, VMR was not correlated with the grade of white-matter lesions. However, these results are not conclusive given the small number of patients in our study. Therefore, future studies should include a larger population of AD patients, and also evaluate cognitive function in more detail (i.e., using instruments additional to the MMSE). In addition, follow-up measurements of VMR and assessments of their correlation with the degree of cognitive decline are warranted.
Several methods have been used to measure VMR. The semiclosed rebreathing method as used in this study is easy to apply to and well tolerated by elderly demented patients, who may be uncooperative. The value of VMR measured by this method is comparable to that obtained by CO2-inhalation and breath-holding techniques.17 In the present study, an adequate CO2 retention of near 50 mmHg or more was obtained in all subjects.
In conclusion, we have shown that VMR is reduced in patients with AD, which may be indicative of the microangiopathy of AD. Screening of cerebrovascular reserve by measuring VMR using TCD could represent a much-needed, reliable, safe, and cost-effective technique for patients at risk of dementia. Future studies should check the validity of these experimental and hypothesis-generating pilot results.


 XML Download
XML Download