

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Blood-injury phobia is a phobia subtype that differs from other specific phobias in that it induces syncope rather than fear or anxiety.1 The phobic response can be triggered by the sight of blood, by sustaining an injury, or by receiving an injection or other invasive medical procedure. The syncope in blood-injury phobia is believed to be of the vasovagal type.2 Transcranial Doppler (TCD) is used to evaluate cerebral blood flow and to differentiate the types of syncope.3 In this report, we present the TCD findings and a favorable outcome of therapy by physical maneuvers in a patient with vasovagal syncope attributed to blood-injury phobia.
CASE REPORT
A 26-year-old man presented with a history of syncope during painful situations. The patient recalled that his first experience of syncope occurred at the age of 15 years when he was spanked on his buttocks as a punishment at school. At age 21, he experienced syncope while undergoing venipuncture at a college clinic, and his third episode occurred on receiving an injection of local anesthetic at a dental clinic.
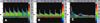
There was no history of cardiac or neurological problems, and no family history of similar symptoms. Physical examination, electrocardiography, and echocardiography findings were all normal. His blood pressure was 120/80 mm Hg, and there was no orthostatic hypotension. While the patient was standing, a TCD scan of the left middle cerebral artery demonstrated a mean cerebral blood flow velocity of 66 cm/s, a peak systolic velocity of 97 cm/s, a diastolic velocity of 37 cm/s, a pulsatility index of 0.89, and a pulse rate of 72 beats/min (Fig. 1-A).
After receiving informed consent, we attempted to reproduce the syncope by venipuncture of the left antecubital vein while the patient was standing, with the needle being withdrawn immediately. After approximately 10 s, the patient felt dizzy, and the systolic blood pressure was unobtainable. At the moment of presyncope, a TCD scan of the left middle cerebral artery showed a decreased mean blood flow velocity (to 46 cm/s), decreased peak systolic velocity (to 75 cm/s), decreased diastolic velocity (to 19 cm/s), decreased pulse rate (to 58 beats/min), and increased pulsatility index (to 1.19) (Fig. 1-B). At approximately 20's after the trigger, the patient was unable to stand and was immediately placed in a supine position. At the time of syncope, the blood pressure and cerebral blood flow were unobtainable due to asystole (Fig. 1-C). Until the presyncope progressed, TCD monitoring showed a more prominent decrease in diastolic blood flow velocity and an increased pulsatility index. Based on the changes in blood pressure, heart rate, and TCD parameters, the patient was diagnosed with vasovagal syncope due to blood-injury phobia.
The patient was scheduled for therapy involving repeated exposure to venipuncture and physical maneuvers once weekly. The physical maneuvers included leg crossing and muscle tensing (Fig. 2-A), which were performed simultaneously. The patient was instructed to cross and contract his legs for the leg crossing maneuver4 and to tense the muscles of his arms, chest, abdomen, and buttocks, without holding his breath for the muscle tensing manuever5 until his prodromal symptoms disappeared. The therapeutic sessions were conducted with the patient standing, and a medical staff member was available to support the patient.
The patient felt faint approximately 30's after the venipuncture during the first session, and thus the session was stopped. His systolic blood pressure decreased from 120 to 70 mm Hg. During the second session, the systolic blood pressure decreased to 80 mm Hg without dizziness at 30's after venipuncture. At approximately 50's after the trigger, the patient felt faint and was placed in the supine position. During the third session, fainting did not develop, the systolic blood pressure did not decrease (Fig. 3), and TCD revealed no significant changes. The patient was instructed to continue practicing these maneuvers at home. It was recommended that, if the physical maneuvers failed to stop his dizziness, the patient should sit or squat while continuing both the leg crossing and muscle tensing maneuvers (Fig. 2-B, and D). The patient was prescribed 25-mg alprazolam and 10-mg propranolol twice a day. Five days after the third session, the patient successfully received a dental procedure without fainting.
DISCUSSION
To the best of our knowledge, this is the first report of TCD findings in a patient with syncope induced by blood-injury phobia. These findings were used to successfully diagnose vasovagal syncope, and the TCD findings were concordant with a previous report of vasovagal syncope with respect to the increased pulsatility index and decreased diastolic blood flow velocity after provocation.3 TCD may also be helpful in the therapeutic management of this condition by allowing simultaneous blood flow monitoring to pre-empt full-blown syncope and accordingly stop the session where necessary.
The most common type of syncope seen in clinical practice is vasovagal, which is also referred to as neurally mediated, vasodepressor, or reflex syncope.6 Vasovagal syncope belongs to the noncardiogenic class of syncope, along with postural orthostatic tachycardia syndrome and orthostatic hypotension.7 In vasovagal syncope, blood pressure is usually maintained initially with compensatory tachycardia, but subsequently drops with bradycardia when patients develop syncope or presyncope.6 Although initial tachycardia was not observed after venipuncture in this patient, hypotension with bradycardia was noted when the patient developed syncope.
The treatment of vasovagal syncope should include avoiding the trigger event. When this is not feasible, the maintenance of central fluid volume and slower changes in posture may be advocated. There is no evidence for the efficacy of drugs in preventing syncope, including beta-adrenergic blockers.8 In blood-injury phobia, repeated exposure to triggers can decrease the associated fear without increasing the heart rate, but physical maneuvers are even more important than the repeated exposure.9 The common physical maneuvers used include crossing the legs and tensing the muscles. Leg crossing involves crossing the legs and contracting the leg muscles while standing,4 and muscle tensing is accomplished by tensing the muscles of the arms, chest, abdomen, and buttocks while maintaining regular breathing.5 Physical maneuvering without repeated trigger exposure can be sufficient to prevent syncope in blood-injury phobia,9 and has also proven to be effective in treating orthostatic hypotension.10 Leg crossing combined with muscle tensing when applied at the onset of prodromal symptoms can prevent or delay syncope.4 The mechanism underlying the success of physical maneuvers as a treatment is unrelated to neural reflex activity.8 Leg crossing produces a rise in cardiac output and blood pressure, while muscle tensing causes an increase in heart rate and an additional rise in blood pressure.11 Leg crossing should therefore be applied as a preventive method during prolonged standing, and muscle tensing would be useful when presyncopal symptoms are experienced.11 Patients who are markedly obese,11 elderly, or who experience disequilibrium should not be encouraged to practice leg crossing. Sitting on a chair or squatting can be used to prevent postural hypotension by increasing venous return and cardiac output10 (Fig. 2-B and D). Hand gripping alone stabilizes blood pressure but it cannot prevent fainting.4 Our experience is that lowering the head also helps one avoid a fainting response (Fig. 2-C). The physical maneuvers are easy to perform, safe, and inexpensive, and should be recommended for treatment4 and subsequent prevention of vasovagal syncope due to blood-injury phobia.


 XML Download
XML Download