

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Striatocapsular infarctions are caused by the simultaneous occlusion of more than one orifice among the immediately adjacent small, long, lenticulostriate arteries. In contrast to the original concept that striatocapsular infarctions occur nearly exclusively as a result of embolic occlusion of the proximal middle cerebral artery (MCA),1-3 a significant proportion of this type of infarction also occur as a result of in situ thrombosis of the MCA. According to previous reports,4-8 the most frequent causes of striatocapsular infarcts are artery-to-artery embolism from the internal carotid artery (ICA; 38%) and cardiogenic embolism (37%), as well as atherosclerotic disease in the MCA at the origin of the lenticulostriate arteries (32%). Furthermore, MCA disease is a relatively common cause of stroke in patients with Asian ancestry,9,10 and is expected to be a more important cause of striatocapsular infarctions.
The identification of stroke subtype is valuable for both practicing clinicians and the optimal design of clinical stroke trials because the etiology of ischemic stroke affects patient management, outcome, and prognosis. 11,12 In addition, the treatment of intracranial atherosclerotic disease may be different from that for extracranial ICA disease13 as well as cardiogenic embolism. However, the TOAST (Trial of Org 10172 in Acute Stroke Treatment) system, which is the most widely used stroke classification, is insufficient for differentiating between in situ thrombotic striatocapsular infarction and ICA disease or cardioembolism, although it exhibits a high agreement between physicians.14,15 Because of concomitant atherosclerotic changes in the proximal vessels or cardiogenic embolic sources and remnants of emboli in MCA ("embolic stenosis"), many striatocapsular infarcts are frequently included in the "undetermined etiology (two or more)" category according to the TOAST classification.
Large striatocapsular infarcts generally exhibit a comma-like shape in coronal section.8 In contrast, small, deep infarctions of the lenticulostriate territory have been found in patients with atherosclerotic MCA disease16-18 as well as those with extracranial embolic sources.19,20 In addition, proximal MCA stenosis is a common cause of small, deep, striatocapsular infarctions in Korean patients, affecting the clinical course and magnetic resonance imaging (MRI) features.21 However, there has been no clear description about the relationship between lesion patterns of acute striatocapsular infarcts and stroke mechanisms.
The advent of diffusion-weighted imaging (DWI) has greatly improved the ability of clinicians to diagnose subtypes of acute ischemic stroke, and the use of DWI / magnetic resonance angiography (MRA) within 24 hours of hospitalization substantially improves the accuracy of the diagnosis of early ischemic stroke subtypes.22 Contrast-enhanced (CE)-MRA is advantageous in displaying detailed vessel anatomy, including that of the aortic arch, and in reducing the appearance of artifacts.23
In the study presented here, we elucidated more accurately the mechanism of stroke with the aid of CE-MRA and aggressive work up for cardiogenic embolic sources, and investigated whether the lesion distribution of acute MCA infarctions involving the striatocapsular region on coronal DWI is associated with different stroke mechanisms.
Go to : 
MATERIALS AND METHODS
We prospectively recruited patients with acute MCA infarction involving the striatocapsular region who were admitted to the Soonchunhyang University Hospital between March 2005 and April 2006. The inclusion criteria included an acute infarction area that was larger than 15 mm on axial DWI and located in the lenticulostriate artery territory with or without infarction in the superficial perforator territory, as defined according to previously published templates.24 Patients with multiple small infarctions in the lenticulostriate territory that were unlikely to be lacunar infarctions were also included. All patients underwent conventional MRI and axial/coronal DWI on a 1.5-T system with echo-planar imaging capability (Sonata, Siemens Medical System) within 3 days of stroke onset. DWI was performed in the three planes with a single-shot, echo-planar, spin-echo pulse sequence with a TR of 2500 ms, a TE of 76 ms, one excitation, and two B values (0 and 1000 s/mm2).
Brain coronal DWI was performed to evaluate the distribution of infarcts in all patients. The high-signal-intensity lesions on coronal DWI were classified into three categories: (1) dominant in the distal territory (DD, Fig. 1-A), (2) distributed equally between the distal and proximal territories (DE, Fig. 1-B), and (3) dominant in the proximal territory (DP, Fig. 1-C). Single lacunar infarctions that were less than 1.5 cm in diameter were excluded (Fig. 1-D). The upper limit of the proximal territory, or the lower limit of the distal territory, was accepted as the exact half of the total length of the perforator (Fig. 2-A) in each section, based on the coronal template of lenticulostriate artery territories (Fig. 2-B).25 After scanning the images of each of the DWI sections, we determined the dominant part by summing each of the high-intensity areas. Coronal DWI was assessed by two readers (K.B. Lee and H.J. Roh) with good interobserver agreement (κ=0.893), and the opinion of a third reader (M.Y. Ahn) was obtained in cases of disagreement.
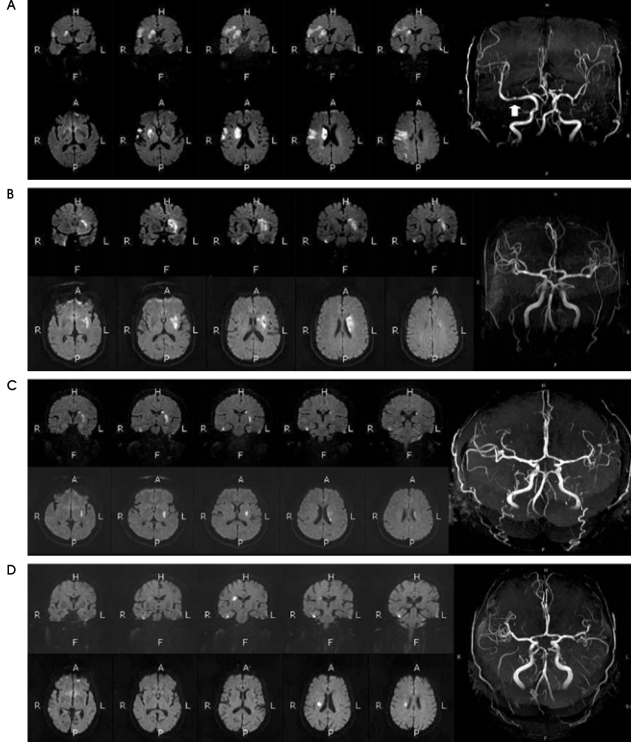 | Figure 1Three types of lesion distribution of acute MCA infarction involving the striatocapsular region on axial/coronal DWI. (A) DD lesions appear as larger, high-intensity areas in the distal lenticulostriate territory, and are associated with MCA M1 stenosis (arrow). (B) DE lesions appear as 'comma-like shape' occupying an area of similar size in both the distal and proximal territories. (C) DP lesions are more prominent in the proximal territory. A typical lacunar infarction (D) which has <1.5 cm oval shape of high intensities on coronal DWI was excluded.
|
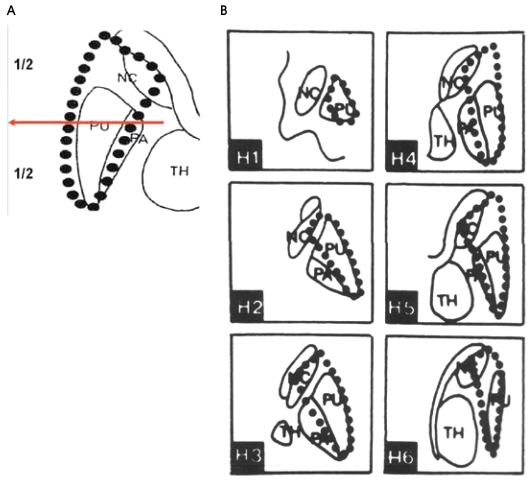 | Figure 2Definition of the boundary line (red arrow) that divides the proximal and distal territories. The line was the exact half of the total length of the perforator in each section (A), based on the coronal template 25 of the lenticulostriate artery territories (B). NC; caudate nucleus, TH; thalamus, PU; putamen
|
We determined the presence of MCA M1 stenosis on CE-MRA using a previously described method.26 A diagnosis of significant (>50%) intracranial and extracranial stenosis was made by two experienced stroke neurologists, and confirmed by a neuroradiologist. We executed tests for proximal embolic sources (transthoracic echocardiography, TTE; transesophageal echocardiography, TEE; Holter monitoring; aortic arch CEMRA) in most patients, and high- and low-risk cardioaortic sources were distinguished using an arbitrary 2% annual or on-time primary stroke risk threshold. Factors associated with a high primary risk for ischemic stroke include left atrial thrombus, left ventricular thrombus, atrial fibrillation, paroxysmal atrial fibrillation, sick sinus syndrome, sustained atrial flutter, recent myocardial infarction (within 1 month), rheumatoid mitral or aortic valve disease, bioprosthetic and mechanical heart valves, chronic myocardial infarction together with a low ejection fraction of less than 28%, symptomatic congestive heart failure with an ejection fraction of less than 30%, dilated cardiomyopathy, and nonbacterial thrombotic endocarditis.27
Strokes were classified according to their underlying mechanism as stroke from proximal embolism (SPE), MCA disease (MCAD), and stroke of undetermined etiology (SUE). For example, because the absence of M1 stenosis is generally considered as recanalization of an embolus, patients without MCA stenosis were classified as SPE independent of evidence of proximal embolic sources, and patients who had M1 stenosis but an unknown proximal embolic source were classified as MCAD. However, patients who had both MCA stenosis and a proximal embolic source were defined as SUE. For these patients, transcranial Doppler (TCD) was performed 0 and 7 days after CE-MRA according to standardized manual of operations. The mean flow velocities of the MCA at depths of 60 and 66 mm were measured on both sides.
All data were analyzed by SPSS 11.0 software (Chicago, IL, USA). The χ2 test and Fisher's exact test were used to compare the distribution of stroke lesions with respect to stroke subtypes. Results are presented as odds ratios as estimates of the relative risk, with 95% confidence intervals. A probability value of P<0.05 was considered statistically significant.
Go to :
RESULTS
The study population comprised 28 male and 19 female patients aged of 62±11.8 (mean±SD) years (range, 37~88 years). Brain coronal DWI and CE-MRA including of the aortic arch were performed on all patients, and TTE, TEE, and Holter monitoring for the proximal embolic source were performed on 47 (100%), 38 (80.9%), and 41 patients (87.2%), respectively. Among the 47 acute MCA infarctions involving striatocapsular regions, 15 (32.6%) were DD lesions, 27 (58.7%) were DE lesions, and 5 (8.7%) were DP lesions. Of the 15 DD lesions, 14 had M1 stenosis (2 with and 12 without a proximal embolic source), and only 1 had no M1 stenosis (without a proximal embolic source). Of the 27 DE lesions, 14 had M1 stenosis (11 with and 3 without a proximal embolic source) and 13 had no M1 stenosis (10 with and 3 without a proximal embolic source). Of the five DP lesions, two had M1 stenosis (one with and one without a proximal embolic source) and three had no M1 stenosis (all with a proximal embolic source; Table 1). DE lesions were the most common type, and they occurred significantly more frequently in the SPE group (P=0.001). In contrast, DD lesions were significantly more common in the MCAD group (P=0.032).
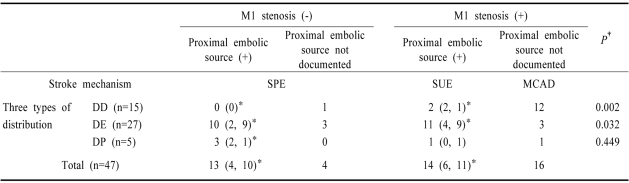
Of those lesions with no M1 stenosis in the SPE group (n=17), 1 was a DD lesion, 13 were DE lesions, and 3 were DP lesions. High-risk cardiogenic embolic sources were detected in ten patients, and ICA embolic sources in four. On the other hand, of those in the MCAD group who had M1 stenosis without a proximal embolic source (n=16), 12 had DD lesions, 3 had DE lesions, and 1 had a DP lesion. In the SUE group, those who had both M1 stenosis and a proximal embolic source, 2 had DD lesions, 11 had DE lesions, and 1 had a DP lesion. Cardiogenic embolic and ICA embolic sources were found in 11 and 6 cases, respectively.
In the two serial TCD scans performed with a 1-week interval in the SUE group, seven patients (50%) showed a reduced or normalized MCA flow velocity. These findings were observed in only two patients in the MCAD group (1.3%; P=0.046).
We compared intracranial MRA images between the SUE and MCAD groups. There were 12 proximal M1 stenoocclusions in the MCAD group, and 4 distal M1 stenoocclusions. However, the SUE group had eight proximal M1 stenoocclusions and seven distal M1 stenoocclusions (P=0.151). There was a tendency toward more frequently occurring abrupt M1 cutoffs in an otherwise normal-appearing artery in the DE group (8/14 patients, 57.1%) than in the MCAD group (3/16 patients, 18.8%, P=0.057). There were 11 patients with other stenotic lesions in the MCAD group, and 4 in the SUE group (P=0.066).
The stroke mechanisms did not different significantly between isolated striatocapsular infarctions (n=18) and MCA infarctions involving the striatocapsular region (n=29). There were 7, 3, and 8 patients with isolated striatocapsular infarction in the SPE, SUE, and MCAD groups, respectively, but 10, 11, and 8 patients had MCA infarction involving the striatocapsular region with concomitant cortical infarction (P=0.263).
Go to :
DISCUSSION
We have demonstrated that visualization of the dominant part of acute infarcts in the lenticulostriate artery territory on coronal DWI can be useful for elucidating stroke mechanisms in striatocapsular infarctions. There is a strong association between DD lesions and MCAD, and between DE lesions and SPE. The location of MCA M1 stenosis was not significantly different between the SUE and MCAD group; however, many cases in the MCAD group could also have been included in the SPE group, because the DE lesions in the SUE group had a tendency toward more frequently occurring abrupt cutoffs on MRA and a higher rate of flow velocity normalization on TCD. Complete recanalization of a prior occlusion by angiographic methods or ultrasound usually supports an embolic cause.27-29
It is not obvious why DD lesions are associated with MCAD, but there are some plausible reasons. Lee et al.30 suggested that MCA internal border-zone infarctions are related to a high degree stenosis of the MCA, while cortical or territory infarctions are correlated with the potential source of cardioembolism. There is controversy regarding the existence of the MCA internal border zone, but it is thought to be located in the region between the superficial perforator and deep perforator territories.24,31,32 However, there are many variables in the territories of the major cerebral arteries,33 and the exact boundary of the distal deep perforator territory and the MCA internal border zone has not yet been determined. Furthermore, a thrombus originating from an MCA atheromatous plaque or a junctional atheroma of a perforating artery is likely to be small and transient,34 resulting in incomplete occlusion of a few perforators and injury to the most vulnerable distal part of the lenticulostriate artery territory or MCA internal border zone. An artery-to-artery embolism from a junctional atheroma would also be possible in this situation.
On the other hand, DE lesions are found frequently in the SPE group. Cardiogenic emboli are usually large and rich in red blood cells, so-called red thrombi.35 These bulky and dense emboli could cause "bunchwise" occlusion of multiple lenticulostriate arteries, resulting in a large striatocapsular infarction. In the same manner, large emboli from ICA stenoses are able to occlude multiple lenticulostriate arteries, but small emboli would be unlikely to result infarction in the lenticulostriate artery territory. DP lesions, which were extremely rare in our study, are not considered as typical striatocapsular infarctions, and maybe attributable to occlusion of some short branches of the main perforating arteries.
There are several weak points to our methods. Firstly, we did not subdivide further the degree of MCA stenosis. Although a few reports discuss the lesion patterns of "angiographic" MCA disease,30,36,37 the degree of intracranial arterial stenosis is changeable13 or recanalizable, and is influenced by proximal embolism. Our approach, which is based on the analysis of lesion location on DWI, is more practical and can be helpful to determine a treatment plan. In addition, there is no previous report in which coronal views of DWI are used in the evaluation of acute striatocapsular infarctions. Coronal views have advantages with respect to the description of lesion shapes and the distribution of lenticulostriate artery territory by nature. Secondly, the exact halfway line that divides the proximal and distal part of the lenticulostriate territory on coronal planes can be somewhat arbitrary. From this viewpoint, a larger cohort should be studied with coronal DWI to obtain more suitable lesion patterns. Finally, another limitation of this study is that intracranial stenoses were evaluated by TCD. Although the MCA flow velocities had reduced in the DE patients from the SUE group, this may have been attributable to mere hemodynamic changes (decreased luxury perfusion).38 Future studies should employ angiography to monitor serial changes in MCA stenoses.
In conclusion, the results of this study suggest that specific distributions of types of lesion, as evaluated by coronal DWI, are associated with specific stroke etiologies in acute MCA infarction involving the striatocapsular region. Identification of coronal DWI lesion distribution may provide early clues as to stroke etiology. Further studies are needed to confirm these observations and to determine whether coronal DWI of these lesions provides important information about stroke mechanisms in striatocapsular infarctions, independent of angiographic findings.
Go to :
 XML Download
XML Download