

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Clinical differences between medial temporal lobe epilepsy (MTLE) and lateral temporal lobe epilepsy (LTLE) have been found in several studies.1-6 MTLE is a well-established condition with a typical semiology and hippocampal sclerosis on MRI, whereas LTLE is relatively poorly characterized. LTLE generally has a less favorable surgical outcome than MTLE, which may be related to inadequate localization and resection of the epileptogenic zone.1 Standard temporal lobe resections usually save the posterior temporal lobe, which includes speech areas. It is difficult to completely resect dominant temporal foci due to the presence of language areas. The presurgical differentiation of posterior temporal lobe seizures from anterior temporal seizures would influence the surgical strategy and improve surgical outcome, particularly in nonlesional cases. This study describes the clinicoelectrical characteristics of patients with anterior LTLE (ALTLE) and posterior LTLE (PLTLE), and compares them with those of MTLE patients.
MATERIALS AND METHODS
1. Patients
LTLE was defined as an epilepsy syndrome fulfilling three criteria: (1) a discrete lesion or ictal onset zone confirmed by invasive study, located exclusively outside the collateral sulcus, (2) absence of hippocampal atrophy or signal changes under magnetic resonance imaging (MRI) when employing 3-mm sections perpendicular to the long axis of the hippocampus, and (3) achievement of good postsurgical outcome (Engel class I or II) for at least one year.7 LTLE was categorized into anterior or posterior LTLE (ALTLE or PLTLE) according to whether the location of the epileptogenic zone was anterior or posterior to the line across the cerebral peduncle (Fig. 1). Patients with a large lesion covering both the anterior and posterior temporal lobes were excluded. 13 patients fulfilled our criteria of ALTLE, and 8 fulfilled the criteria of PLTLE, out of 92 consecutive patients who were operated upon for LTLE between 1994 and 2001 (Table 1). All patients became seizure-free after the operation except for 2 PLTLE patients who experienced very occasional seizures (Engel Class II). MTLE was defined when hippocampal sclerosis was detected on MRI in the absence of other structural lesions, and the patient had been seizure free for at least one year after standard anterior temporal lobectomy with amygdalohippocampectomy. Over the same period, 21 patients that were randomly selected from 204 MTLE patients fulfilled the criteria.
All patients received presurgical evaluations including video-EEG monitoring, MRI, Fluoro-deoxyglucose (FDG) PET, ictal SPECT if possible, and Wada test. 4 ALTLE patients, 6 PLTLE patients, and 1 MTLE patient undertook intracranial EEG recording. 6 ALTLE patients, 5 with PLTLE, and 14 with MTLE received ictal SPECT. 9 ALTLE patients received an anterior temporal lobectomy with amygdalohippocampectomy and four ALTLE patients received anterior temporal neocortical resection only. 5 PLTLE patients recieved lesionectomy, 3 PLTLE patients received additional anterior temporal lobectomy with amygdalohippocampectomy because of rapid propagation of ictal rhythm to the anterior temporal areas. The MTLE patients received anterior temporal lobectomy to a variable extent (3.5~5 cm) depending on the side of epileptogenic lobe and amygdalohippocampectomy. Gross and microscopic tissue analyses were performed in all cases.
2. Clinical characteristics
Demographic data, age at onset of afebrile seizure, frequency of seizure, auras, and outcomes were retrospectively reviewed from medical records. Auras were classified as epigastric, psychic, memory-related, auditory, vertigo, visual, or other. Epigastric aura included epigastric uprising sense, nausea, vomiting, and discomfort in the epigastric area. Psychic aura included anxiety, fear, forced thinking, and a feeling of unreality. Memory-associated aura included déjà vu, strange feelings, flashback, and panoramic experience. Auditory aura included tinnitus, deafness, and hallucination.
3. Video-EEG monitoring
All patients were monitored using continuous video-EEG monitoring using scalp electrodes according to the international 10/20 system, and with additional anterior temporal electrodes (T1 and T2). Antiepileptic medications were discontinued during the monitoring. Total 107 seizures (34 seizures in 13 ALTLE patients, 19 in 8 PLTLE patients, and 54 in 21 MTLE patients) were analyzed. Ictal onset was defined by earlier sign of symptom and EEG. Ictal onset by symptom was defined as the time when a patient first experienced an aura, or when altered responsiveness or abnormal movement was first noticed. Ictal onset based on EEG was defined as the onset of rhythmic activity. The end of a seizure was defined as the end of the ictal EEG rhythm. Initial symptoms, ictal behaviors, duration of complex partial seizure, and latency to the onset of generalized tonicclonic seizure (GTCS) were analyzed. We classified ictal behaviors as follows: oroalimentary automatism, hand automatism, dystonia of the upper extremity, staring or behavioral arrest, looking around, body shifting, hyperactivity, version, facial twitching, limb clonic movement, and limb tonic movement. Dystonia and tonic movement were differentiated by a twisting component. Version was defined as a forced turning of the head or eyeball. Ictal EEGs were reviewed by one of the authors (S.K.L.) blinded to patient information, including semiology and resection site. A total of 110 ictal EEGs of adequate quality (30, 22, and 58 EEG recordings of the 13 ALTLE, 8 PLTLE, and 21 MTLE patients, respectively) were analyzed. Ictal EEGs were analyzed with respect to location and rhythm. The ictal pattern distributions were classified as follows8:
Discrete pattern: the amplitude of the initial ictal rhythm was 200% higher in one electrode than in the others.
Regional pattern: the amplitude of the initial ictal rhythm was 200% higher in two adjacent electrodes than in the others.
Lobar pattern: the amplitude of the initial ictal rhythm was 200% higher in three adjacent electrodes than in the others.
Hemispheric pattern: the amplitude of the initial ictal rhythm was 200% higher in multiple electrodes over multiple lobes in one hemisphere than in the others.
Bilateral pattern: the initial ictal rhythm occurred bilaterally.
Falsely localized pattern: the initial ictal rhythm started at lobes not in the epileptogenic area.
Focal and regional patterns originating from temporal electrodes were subdivided into anterior temporal and posterior temporal onset. Ictal onset from T1 and T3 electrodes (or T2, T4) was classified as anterior temporal regional onset pattern, whereas ictal onset from T5 and T3 (or T6, T4) electrodes was classified as posterior temporal regional onset pattern. F7, T1, and T3 (or F8, T2, and T4) ictal onset was classified as anterior temporal regional onset pattern (not lobar).
All initial ictal rhythms were also classified on the frequency spectrum.
4. Statistical analysis
We used χ2 analysis and Fisher's exact test for categorical variables to evaluate the significance of differences in the occurrence of features between the groups. Duration of seizure and age were compared using ANOVA or the Kruskal-Wallis test for continuous variables. Statistical significance was accepted when P< 0.05.
RESULTS
1. Clinical characteristics
The demographic data are summarized in Table 2. Age, sex, side of lesion, onset age of afebrile seizure, and seizure frequency did not differ significantly between the groups.
Epigastric aura was less common in PLTLE and ALTLE than MTLE, but not significantly (P=0.161, Fisher's exact test). Psychic auras were absent in PLTLE. Memory-associated aura did not differentiate the site of lesion. Visual and vertiginous auras were reported in PLTLE, and auditory auras were reported in both ALTLE and PLTLE. Some patients had more than one type of aura (Table 3).
2. Ictal behavior
Initial oroalimentary automatism was not observed in PLTLE, which distinguished it from ALTLE and MTLE. Initial hypomotor symptoms such as staring and behavioral arrest were more frequent in PLTLE (P<0.001, χ2 analysis). Initial hypermotor activity was observed in only one ALTLE patient. Version and GTCS occurred more frequently in ALTLE and PLTLE than in MTLE (version: P=0.005, χ2 analysis; GTCS: P=0.001, χ2 analysis). Looking around was more frequent in MTLE than in ALTLE and PLTLE (P=0.004, Fisher's exact test). No differences were observed in the occurrences of oroalimentary automatism, hand automatism, hypermotor activity, body shifting, dystonia, facial twitching, limb clonus, or tonic posturing (Table 4). Secondary GTCS (Table 5) occurred significantly earlier in PLTLE than in ALTLE or MLTLE (P<0.001, Kruskal-Wallis test).
3. Ictal EEG
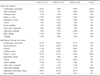
Focal or regional EEG ictal onset was observed in 43%, 59%, and 28% of ALTLE, PLTLE, and MTLE patients, respectively. The most common ALTLE pattern was anterior temporal regional onset (11 of 30 seizures). However, 2 ALTLE seizures originated from the posterior temporal electrodes, and 7 were falsely localized to the contralateral temporal (5 seizures) or the ipsilateral frontal lobe (2 seizures). The most common pattern of PLTLE was posterior temporal onset (7 of 22 seizures). There were 5 PLTLE seizures that originated from the anterior temporal electrodes, and 2 were falsely localized to the ipsilateral frontal lobe. MTLE had rather diffuse ictal onset. There were 11, 15, and 11 seizures of the lobar, hemispheric, and bilateral patterns, respectively. Ictal onset was confined to the anterior temporal electrodes in 15 MTLE seizures and confined to the posterior temporal electrodes in 1 MTLE seizure (Table 6).
In all types, the most common initial ictal rhythm was rhythmic theta. Fast activities of the alpha or beta range were more common in PLTLE and ALTLE than in MTLE (P=0.002, χ2 analysis); beta activity was not observed in MTLE (Table 6).
DISCUSSION
Some of the previously employed resective surgical procedures for LTLE have included amygdalohippocampectomy. Clear guidelines of surgery for LTLE were absent, and seizure reduction or cure by anterior temporal lobectomy in remote posterior lesion was reported in several studies.9,10 We included the anterior temporal area because of the rapid propagation of ictal rhythms from the posterior to anterior temporal area. It may remove the critical sites for full seizure development and spreading.11 We now perform only neocortical resection for LTLE.
Epigastric auras are considered to be typical of MTLE and rare in LTLE.12,13 Our results showed a similar tendency and there was no difference between ALTLE and PLTLE in this respect. Visual and auditory hallucinations have been considered indicators of LTLE.13,14 Both ALTLE and PLTLE were associated with auditory auras, and 1 PLTLE patient had visual auras in our series. No MTLE patient had visual or auditory auras. The anatomy of auditory auras, including deafness and hallucination, have been incompletely studied, although the superior and posterior parts of the temporal lobe have been reported responsible.15 It has been reported that epileptic activation of the superior and posterior parts of the temporal lobe (posterior to primary auditory cortex) might induce a sense of disequilibrium.16
The location of experiential phenomena, including emotion and memory-associated auras, were not established. Penfield localized this to the lateral temporal lobe,17 and Gloor et al. localized it, by electrical stimulation, to the medial temporal lobe.18 The issue has not been discussed to the point of differentiating anterior and posterior lateral temporal lobes. We found psychic auras in ALTLE and MTLE, but not in PLTLE.
The most common initial symptoms were oroalimentary and hand automatism in ALTLE and MTLE, and hypomotor symptoms, such as staring or arrest, in PLTLE. Oroalimentary19 and hand automatism5 have been reported to occur more frequently in MTLE than in LTLE. However, an analysis of the classification of LTLE to ALTLE and PLTLE reveals that the difference is not between medial and lateral locations but between anterior and posterior locations.
GTCS occurred significantly earlier in PLTLE. It was reported that interhemispheric propagation times were significantly longer in patients with hippocampal sclerosis than those without.20 Symptomatology, beginning with behavioral arrest and progressing to motor convulsion, has been suggested to characterize posterior temporal seizures, but no comparison with anterior temporal seizures has been made.21 Rapid generalization in PLTLE reflects the close connectivity of the posterior temporal and frontal lobes.
Initial ictal scalp EEG was of limited value in differentiating ALTLE and PLTLE because some seizures with a focal or regional ictal pattern were mislocalized to the anterior or posterior temporal electrodes, and many seizures had rather diffuse ictal patterns. The confident differentiation of MTLE and LTLE has been reported to be impossible.2,3,6 Focal or regional ictal EEG patterns were reported to be 37% in LTLE and 42% in MTLE.2 A localized (less than lobar) ictal LTLE pattern was reported in 43~84% of patients.3,4,8 There are reports of a regular 5~9 Hz inferotemporal rhythm as a specific form of MTLE and a 2~5 Hz lateralized activity as a frequent form of LTLE.22 However, more recent studies suggest that fast activity is more specific for neocortical epilepsies and a reflection of the proximity of the epileptic zone to the recording electrodes,8,23 which supports our result.
Differentiation of temporal lobe epilepsy subtypes has been a matter of interest, but only a few studies exist. In the case of LTLE, resective surgery is not readily done and the surgical outcome is relatively poor because of incomplete resection considering language function; the lesions are often of indefinable extent, which this may underlie the absence of large-scale studies of LTLE, especially PLTLE. Our work is the first comparative study on ALTLE and PLTLE using strict diagnostic criteria.
We were unable to find any semiological or EEG characteristics that differentiated the groups, but some tendencies were observed between them. The absence of initial oroalimentary automatism, frequent hypomotor onset, and early generalization are characteristics of PLTLE. ALTLE shares many characteristics with MTLE.






 XML Download
XML Download