

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epilepsy is one of the most common neurologic disorders, and is estimated to affect over 50 million people worldwide.1 Excluding a few patients with intractable epilepsy, who can be treated surgically, most require long-term or lifetime medication. Evidence has emerged over the past few decades that the prolonged use of antiepileptic drugs (AEDs) may be associated with a wide range of chronic adverse effects, including metabolic and endocrine disturbances, organ toxicity, cognitive dysfunction, and psychiatric problems.2345 Several recent studies have also revealed that long-term exposure to AEDs may play a pivotal role in the pathogenesis of atherosclerosis in patients with epilepsy.678
As a chronic inflammatory disease, atherosclerosis is characterized by remodeling of the arterial wall that may progress unnoticed or present as acute vascular events. A larger carotid artery intima-media thickness (CA-IMT) as measured noninvasively by ultrasonography is considered an early surrogate marker of atherosclerosis,910 and previous studies have explored the association of the use of AEDs with increases in CA-IMT. However, the results remain controversial, with some studies678 suggesting that AEDs may increase CA-IMT in epileptic patients, and others111213 finding no significant relationship between AEDs and CA-IMT.
To the best of our knowledge, no previous meta-analysis has addressed the effect of AEDs on CA-IMT in patients with epilepsy. We therefore attempted to establish some consensus by performing a meta-analysis that assessed the association between the use of AEDs and CA-IMT in epileptic patients.
METHODS
Study selection
A systemic computerized search was conducted according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines.14 The present authors (Q.L.L., C.H.S., and Y.Z.) independently searched relevant articles in NCBI (PubMed), ISI Web of Knowledge, EMBASE, and the Cochrane Library databases up to February 2017. No language restriction was applied. The following search terms were used: “epilepsy”, “anticonvulsants”, “antiepileptic drugs”, “carbamazepine”, “valproic acid”, “phenobarbital”, “phenytoin”, “benzodiazepines”, “oxcarbazepine”, “lamotrigine”, “topiramate”, “levetiracetam”, “gabapentin”, “atherosclerosis”, “intima media thickness”, and “intimal medial thickness”. The applied search strategy is detailed in the Supplementary Materials (in the online-only Data Supplement). We retrieved all relevant articles and searched their reference lists to identify as many additional studies as possible.
Eligibility criteria
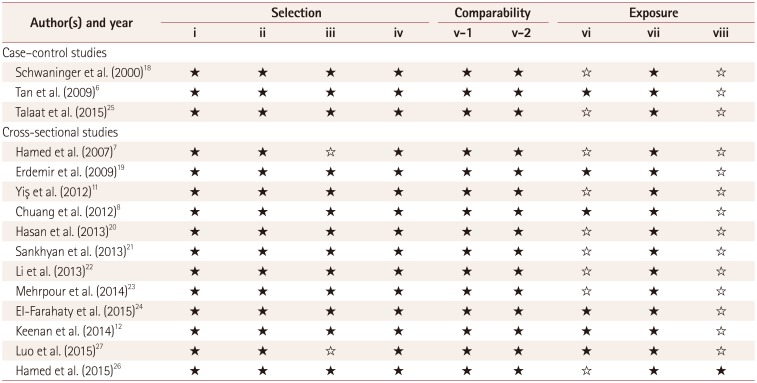
Studies were included if they met the following criteria: 1) original data obtained in epidemiologic studies, and included healthy controls, 2) case-control, cross-sectional, or cohort studies that evaluated the association between AEDs and CAIMT in epileptic patients, 3) exposure to AEDs, 4) the outcome was CA-IMT quantified as the mean with standard deviation (SD) or the median with interquartile range (IQR), and 5) consistent with at least six Newcastle-Ottawa Scale criteria,15 which is an eight-item instrument with up to nine possible points, and was developed to assess the quality of observational studies for inclusion in systematic reviews and meta-analyses (Table 1). All of the present analyses were based on previous published studies, and so ethical approval and patient consent were not required.
Data extraction
All of the identified studies were evaluated and examined carefully by two of the authors (Q.L.L. and C.H.S.), with discrepancies discussed and resolved by the third author (Y.Z.). The following data were collected for each study: authors, publication year, country, study design, population, age, sex, AEDs, exposure duration, and CA-IMT in epileptic patients and healthy controls.
Data analysis
If the CA-IMT was reported as median and IQR values, these were converted into mean and SD values using the method described by Hozo et al.16 If the left and right CA-IMT values were given separately, they were converted into a mean CA-IMT using mathematical formulas.17 Based on age distributions, the studies were stratified into an adult group (≥18 years) and a child group (<18 years).
The data of interest were analyzed as effect measures using the mean difference (MD). Statistical heterogeneity was assessed using the I2 statistic, and p<0.10 was considered significant. Potential inconsistency was qualified with the I2 statistic, which indicates the proportion of variability across studies rather than the sampling error: a value of 0% indicates no observed heterogeneity, and large values indicate increasing heterogeneity. If substantial heterogeneity was detected, we performed the analysis using a random-effects model with the DerSimonian and Laird method; otherwise a fixed-effects model was used.
Sensitivity analysis was also conducted by excluding each study individually and recalculating the combined estimates for the remaining studies to assess the influence of an individual result on the pooled estimate. Egger's test and Begg's test were applied to evaluate publication bias, with p<0.05 considered to indicate the existence of significant publication bias. All of the data analyses were performed using STATA (version SE 12.0, Stata, College Station, TX, USA).
RESULTS
Study characteristics
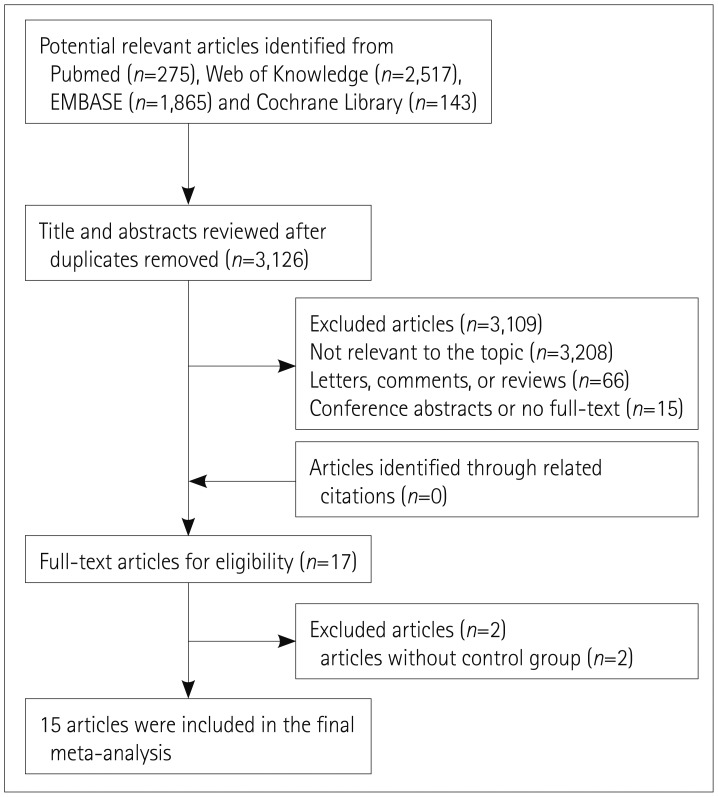
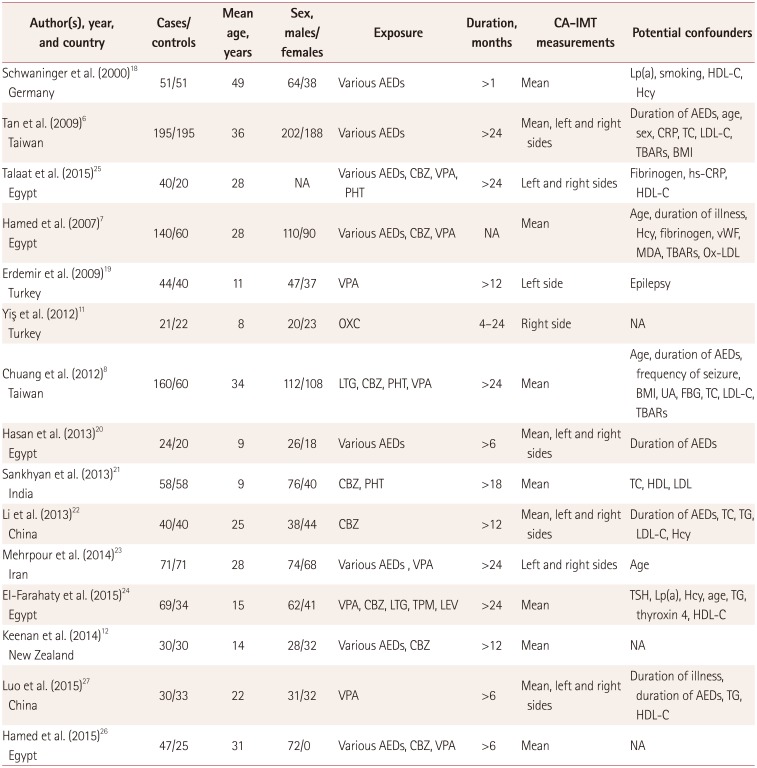
As indicated in Fig. 1, 15 studies678111218192021222324252627 were included in the final analysis. The characteristics of the individual studies are presented in Table 2. The 15 studies involved 1,775 participants and detected the association between exposure to AEDs and CA-IMT: 3 were case-control studies61825 and 12 were cross-sectional studies.7811121920212223242627 Eight of the 15 studies produced results for adults,6781822232526 while 5 produce results for children.1112192021 Eight studies78122122242526 involving 540 participants investigated the association between carbamazepine (CBZ) monotherapy and CA-IMT: 5 for adults,78222526 2 for children,1221 and 1 for both.24 Eight studies78192324252627 involving 550 participants investigated valproic acid (VPA) monotherapy: 5 for adults,78232526 1 for children,19 and 2 for both.2427 Three studies82125 evaluated CA-IMT in 184 patients receiving phenytoin (PHT) monotherapy (184 participants) and two824 evaluated CA-IMT in 131 patients receiving lamotrigine (LTG) monotherapy. Studies involving three AEDs (levetiracetam,24 oxcarbazepine,11 and topiramate24) are not reported on below since the number of studies was insufficient.
Use of AEDs and CA-IMT
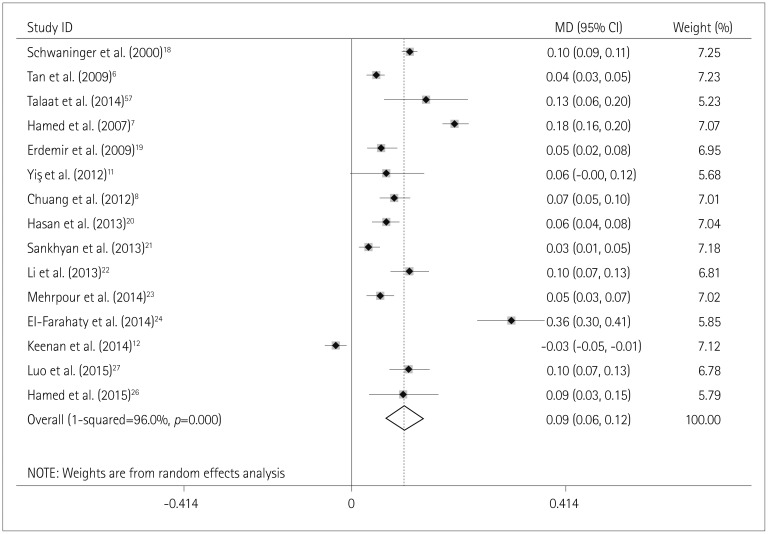
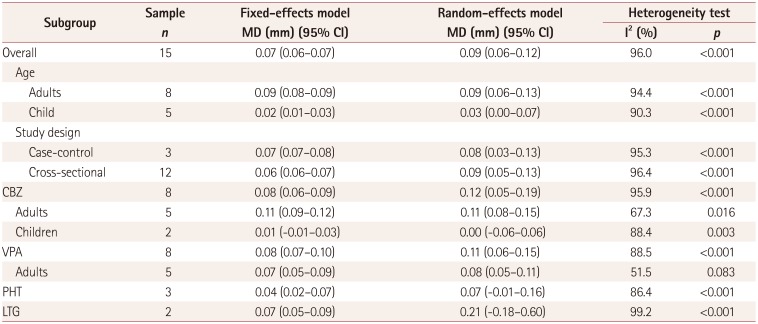
The overall CA-IMT was significantly larger in epileptic patients receiving AED therapy [MD=0.07 mm, 95% confidence interval (CI)=0.06–0.07 mm; p_heterogeneity<0.001, I2=96.0%]. Given the underlying heterogeneity, we reevaluated the MD in the random-effects model, which changed it to 0.09 mm (95% CI=0.06–0.12 mm) (Fig. 2). Subgroup analyses were performed by age (adults vs. children) and study design (case-control vs. cross-sectional studies). The MD in the random-effects model was similar in the subgroup of adults (MD=0.09 mm, 95% CI=0.06–0.13 mm; I2=94.4%), but was not significant in the child group (MD=0.03 mm, 95% CI=0.00–0.07 mm; I2=90.3%). Case-control studies indicated that CA-IMT was significantly larger among users of AEDs (MD=0.08 mm, 95% CI=0.03–0.13 mm; I2=95.3%), with cross-sectional studies producing a similar result (MD=0.09 mm, 95% CI=0.05–0.13 mm; I2=96.4%) (Table 3). After excluding three studies71118 with an AED exposure duration of less than 6 months or no duration information, the MD of CA-IMT in the random-effects model changed to 0.08 mm (95% CI=0.05–0.11 mm), which was similar to the original result of 0.09 mm (95% CI=0.06–0.12 mm; I2=94.5%).
Heterogeneity was still present after performing subgroup analyses by age and study design, and so we recalculated the combined results by excluding one study per iteration in order to perform a sensitivity analysis. The study-specific MD ranged from 0.07 mm (95% CI=0.04–0.10 mm) with the omission of the study of EI-Farahaty et al.24 to 0.10 mm (95% CI=0.07–0.13 mm) with the omission of the study of Keenan et al.12
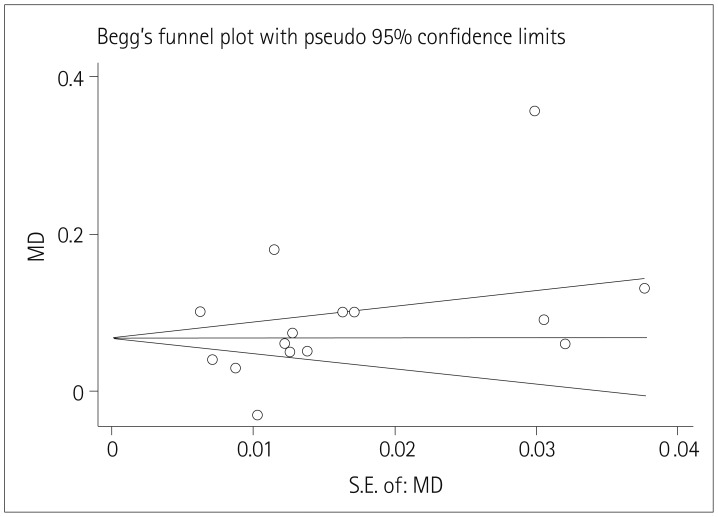
No publication bias was detected using Egger's test (p=0.289) and Begg's test (p=0.235), and Begg's funnel plot appeared to be symmetrical (Fig. 3).
Specific AEDs and CA-IMT
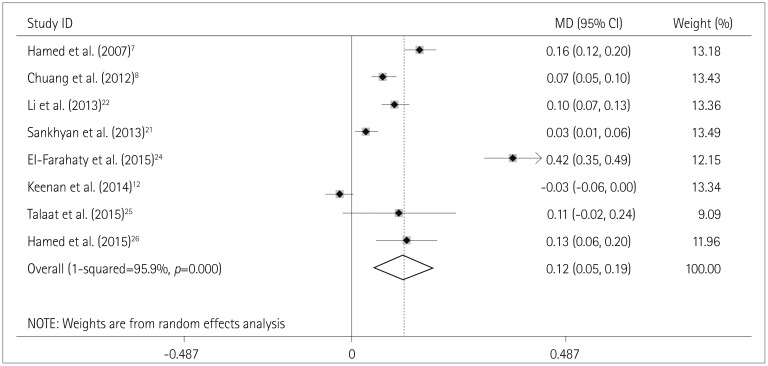
Compared to the control group, it was found that CA-IMT was significantly larger in patients on CBZ monotherapy (MD=0.12 mm, 95% CI=0.05–0.19 mm; p_heterogeneity<0.001, I2=95.9%) (Fig. 4). In the stratified analysis, the pooled MD was 0.11 mm (95% CI=0.08–0.15 mm) in the adult group and 0.00 mm (95% CI=-0.06–0.06 mm) in the child group; the latter was not statistically significant (Table 3).
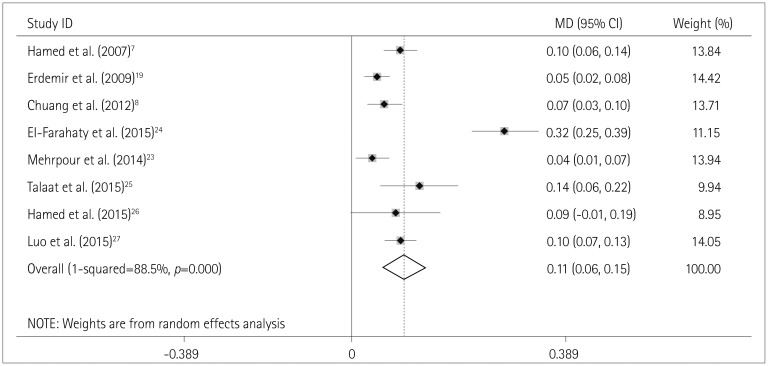
Epileptic patients receiving VPA monotherapy also exhibited a larger CA-IMT (MD=0.11 mm, 95% CI=0.06–0.15 mm) (Fig. 5). The MD was similar in adult patients (MD=0.08 mm, 95% CI=0.05–0.11 mm), while no significant result was observed in children (Table 3).
CA-IMT was not significantly elevated in patients receiving PHT monotherapy (PHT: MD=0.07 mm, 95% CI=-0.01–0.16 mm). For the epileptic patients receiving LTG monotherapy, CA-IMT was significantly larger in the fixed-effects model (MD=0.07 mm, 95% CI=0.05–0.09 mm; p_heterogeneity<0.001, I2=99.2%) but not in the random-effects model (MD= 0.21 mm, 95% CI=-0.18–0.60 mm) (Table 3).
DISCUSSION
This meta-analysis of 15 studies involving 1,775 epileptic patients found that the use of AEDs was associated with a larger CA-IMT, with an MD of 0.09 mm (95% CI=0.06–0.12 mm). The result after stratification by age was similar in adult patients but not in children. Regarding specific AEDs, the use of CBZ or VPA monotherapy had a significant effect on CA-IMT, while PHT did not and the result for LTG was inconclusive. However, these findings must be interpreted with caution due to the presence of significant heterogeneity.
The results obtained in this study suggest that the use of AEDs is associated with CA-IMT in patients with epilepsy. As an early indicator of atherosclerosis, CA-IMT has been linked to many vascular outcomes, including cardiovascular and cerebrovascular events. A Framingham offspring study involving 2,965 participants indicated that the adjusted hazard ratio (HR) for cardiovascular disease with an increase of 1 minus SD (0.13 mm) in CA-IMT was 1.13 (95% CI=1.02–1.24).9 Hermann and colleagues followed 3,669 initially stroke-free subjects for over 5 years, and showed that the HR for stroke per 0.1 mm of thickening in CA-IMT was 1.20 (95% CI=1.01–1.44).10 It can be inferred that exposure to AEDs may be related to an increased risk of atherosclerosis and vascular events in adult epileptic patients, which is consistent with previous findings.282930
However, the role of AEDs in the pathogenesis of atherosclerosis is not fully understood. As described below, three predominant explanations have been suggested. Firstly, long-term AED therapy can result in dyslipidemia, with elevated serum levels of total cholesterol, low-density lipoprotein cholesterol (LDL-C), and lipoprotein a.61821 LDL-C is known to play an important role in the atherosclerotic process by increasing endothelial permeability, the retention of lipoproteins within the intima of blood vessels, the recruitment of inflammatory cells, and the formation of foam cells,31 and thereby contributes to an increase in CA-IMT. Secondly, hyperhomocysteinemia may partial explain atherosclerosis, which could increase the expression of tumor necrosis factor, enhance oxidative stress, and induce a proinflammatory vascular state that might contribute to the development of atherosclerosis.32 Several studies have found that enzyme-inducing AEDs may induce hyperhomocysteinemia by affecting the liver-enzyme induction of folate and vitamin B12.3334 Also, a recent study demonstrated that VPA may be associated with elevated serum homocysteine levels in epileptic patients (both adults and children), probably by impairing the intestinal absorption of folic acid and directly interfering with the metabolism of folic acid coenzymes.193536 Thirdly, serum C-reactive protein (CRP), which is a marker of inflammation, was found to be elevated in epileptic patients receiving AEDs.625 Previous studies have already indicated that CRP can promote inflammation and atherosclerosis by affecting monocytes and endothelial cells and increasing the activity of plasminogen activator inhibitor-1.32
The stratified analysis performed in the present study revealed that the CA-IMT was significantly larger in adult patients receiving AED therapy but not in children, which further weakened the overall MD. We speculate that this agerelated difference may be due to three factors: Firstly, studies have suggested that age is an independent risk factor for atherosclerosis, since arterial plaque caused by other intrinsic and extrinsic factors accumulates with aging.32 The study of Cleary et al.37 indicated that late-onset seizures can be considered to be a predictor of stroke, and so it was suggested that AEDs may play an important role in subsequent stoke particularly among the aged, which was consistent with our results. Secondly, as mentioned above, low folate and vitamin B12 levels (which lead to hyperhomocysteinemia) contribute to the atherosclerotic process.32 Given that folate and vitamin B12 levels decline with age,38 it is reasonable to speculate that children receiving AEDs are less likely to experience hyperhomocysteinemia and atherosclerosis. Thirdly, the sample for the child group was relatively small, which indicates the need for further researches.
Regarding specific AEDs, CBZ, or VPA monotherapy was associated with a larger CA-IMT in patients with epilepsy. As traditional liver enzyme-inducing AEDs, both CBZ and PHT should increase CA-IMT, while PHT is not related to a larger CA-IMT. The negative result for PHT may be explained by the smallness of the sample and the large heterogeneity. LTG is a newer-generation AED that does not exert an enzyme-inducing effect and does not increase the serum homocysteine level,39 and so might play a minor role in the atherosclerotic process. However, the result for LTG was inconclusive since only two studies were included in the present meta-analysis; further studies of these AEDs were therefore needed. Most of the newer AEDs such as lacosamide, brivaracetam, perampanel, and eslicarbazepine do not appear to exert negative metabolic influences, including atherosclerosis.404142 No researches have focused on the relationship between these newer AEDs and CA-IMT, and so relevant studies are urgently required.
Some limitations of this study should be considered. Firstly, since our results were based on observational studies, all of the possible cofounders might not have been controlled sufficiently. A particular concern relates to whether epilepsy itself or the prescribed AEDs plays a role in atherosclerosis. Because a healthy population was included in these studies as control groups, we were not able to accurately discriminate the effect of epilepsy and AEDs on CA-IMT. This could have exaggerated the effects of AEDs on CA-IMT and atherosclerosis. Future studies should pay more attention to comparing between epileptic patients taking and not taking AEDs. Secondly, we observed substantial heterogeneity in the results among all of the included studies and also within stratified subgroups. We assume that this was due to heterogeneity in the CA-IMT measurement methods employed in the various studies. However, the results of the sensitivity analysis were quite similar to previous results, which would increase the reliability of the present study. Thirdly, we converted variables that had nonnormal statistical distributions (calculated as median and IQR values) into normally distributed variables (calculated as mean and SD values) using the method reported by Tan et al.,6 which may have introduced bias. Finally, the duration of exposure to AEDs differed from 1 month to longer than 2 years across the studies, which could have exerted unknown effects on our results.
The present meta-analysis has provided insights into AEDs by showing that the use of AEDs by epileptic patients was associated with a larger CA-IMT and atherosclerosis, particularly among adult patients. Moreover, two AEDs (CBZ and VPA) were observed to exert significant effects on CA-IMT. The findings indicate that neurologists and epileptologists prescribing AEDs should be aware of potentially unfavorable effects, especially in patients at a high risk of vascular events.
 XML Download
XML Download