

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Headache is one of the most common complaints in pediatric neurology clinics. Headache is experienced by 40–50% of 7-year-olds and about 80% of adolescents.1 Migraine is the most common type of headache to present to a primary care provider or neurologist for evaluation, with a prevalence of around 3% in preschoolers that increases to 8% in males and 20% in females when reaching adolescence.234 The prevalence of migraine among school children was reported to be 8.7% in South Korea.5 Migraine frequently affects daily life, making it difficult for children to play with their friends or participate in routine daily activities. It can be a significant problem in school-aged children because frequent absences and early dismissals from school interfere with their academic achievement and social interaction.6 Treatment of migraine includes lifestyle modification and acute abortive or prophylactic treatment depending on the disease severity. Many patients can be successfully treated with either acute symptomatic treatment or lifestyle modification, but about 30% of patients who have frequent or disabling attacks require prophylactic medication.7 Prophylactic treatment usually involves flunarizine, topiramate, valproic acid, propranolol, or amitriptyline, and has been shown to be effective.891011121314
Various prophylactic agents can be applied in pediatric migraines, and their efficacy in reducing the headache frequency by at least 50% ranges between 60% and 90%,3 which means that prophylactic agents show little effect in 10–40% of patients. However, there are no clear recommendations for the choice of a specific agent for individual patients. A better understanding of the factors that affect responses to prophylactic treatment can help neurologists to choose optimal medications and reduce treatment failures. Unfortunately, the few studies that have investigated these factors related to treatment responses have produced conflicting results. Moreover, these studies have only been conducted in adult populations. Based on this background, the present study investigated the characteristics of migraine and associated symptoms with the aim of identifying the predictive factors for a response to prophylactic therapy using topiramate in pediatric patients.
Go to : 
METHODS
This study was approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (SNUBH) (IRB No. B-1511-324-11). Patients diagnosed with migraine at SNUBH between January 2005 and December 2014 were initially screened using an electronic medical database warehousing program. Migraine with or without aura was diagnosed according to criteria in the second edition of the International Classification of Headache Disorders (ICHD), based on the nature, duration, aura, and associated symptoms of the headache (nausea, vomiting, photophobia, and phonophobia), and findings from neurological examinations.15 We included the patients who were at least 7 years old and able to understand and describe their symptoms adequately. Patients who received topiramate prophylaxis for more than 3 months were included. The following exclusion criteria were applied: 1) low headache frequency (<2 episodes per month), 2) concurrent use of analgesics due to reasons other than a headache, 3) receiving additional medication for migraine prophylaxis within 3 months after starting topiramate prophylaxis, and 4) a period of discontinuation of topiramate prophylaxis within the first 3 months after therapy initiation for any reason. In total, 113 patients who met the above criteria were included, and they had formed part of the patient cohort in a previous study.10 More detailed information about patient selection is provided in Fig. 1.

Electronic medical records were reviewed retrospectively. Information regarding sex, age at onset, age at diagnosis, the headache duration, intensity, and average frequency per month, impairment of daily activities, family history, and presence of associated symptoms at the first outpatient visit were collected as baseline data. Headache intensity was recorded using a Numeric Rating Scale (NRS), with 0 points indicating no pain and 10 points indicating the worst possible pain. We asked the patients or their parents if the patient experienced impairment of daily activities at the initial visit that resulted in absence from school or not participating in activities such as sports, playing with their friends, or reading within 3 months due to headache. The family history was considered to be positive if the headache history (headache duration, frequency, and associated symptoms) in any first-degree relative was consistent with a migraine diagnosis. The associated symptoms taken into account included nausea, vomiting, photophobia, phonophobia, dizziness, and visual symptoms. Dizziness was defined as being present when the patient complained about dizziness associated with migraine and when there was no vertigo or other neurological findings in the physical examination. Dizziness was not of whirling type and it was aggravated by head shaking and body movement in almost all of the patients. Visual symptoms included scotoma, flickering lights, and blurred vision, and they were similar to visual aura. However, the symptoms lasted for shorter than 5 minutes or longer than 60 minutes after the onset of headache, which differed from the criteria for visual aura in the second edition of ICHD.15
Patients with at least 10 migraines per month were considered for prophylactic treatment, in accordance with previous recommendations.161718 Patients who experienced fewer than 10 migraine episodes per month but still suffered from severe disturbance in their daily activities and thus willing to receive prophylaxis were also included.
Treatment was started with topiramate at 1 mg/kg daily as a single dose before sleep. Each patient kept a headache diary during the study period, which was used to evaluate the treatment response to topiramate. A positive response was defined as a reduction in headache frequency of more than 50% compared to baseline. The topiramate dosage was increased in increments of 50% of the previous dosage if the migraine frequency was not reduced by 50%. Any increase in the dosage was decided after at least 1 month of treatment, and the maximum allowed dosage was 100 mg/day. A patient was classified as a nonresponder if the frequency reduction did not reach 50% after receiving topiramate for 3 months.
We considered the following factors as possible predictors of treatment response: sex, age at onset, age at diagnosis, the duration, intensity, and monthly frequency of headache, impairment of daily activities, family history, and presence of associated symptoms (nausea, vomiting, photophobia, phonophobia, dizziness, and visual symptoms). We analyzed the above predictors between the responder and nonresponder groups. Sex, intensity of headache (NRS score ≥6 vs. <6), impairment of daily activities, family history, and associated symptoms were classified as categorical variables, and the other variables were classified as continuous variables for the statistical analysis. Since the headache intensity scored using the NRS was not a continuous variable, it was analyzed as a categorical variable.
Categorical variables were analyzed using the chi-square test or Fisher's exact test, while continuous variables were analyzed using the independent-samples t-test. Ordered logistic regression analysis was performed to exclude confounding effects between variables to improve the analysis precision. The response rate was divided into the following four groups for the ordered logistic regression: 0–25, 25–50, 50–75, and 75–100%. The results were analyzed using SPSS software (version 18.0, SPSS Inc., Chicago, IL, USA), and a p value less than 0.05 was considered to be statistically significant.
Go to :
RESULTS
The 113 patients comprised 43 (38.1%) males and 70 (61.9%) females. They were aged 11.8±2.8 years (mean±standard deviation, range=7.1–18.7 years) at diagnosis and 10.3±2.8 years at disease onset, and their duration of topiramate treatment was 8.3±5.1 months. The duration of disease was 17.3±15.8 months and the average headache duration was 6.3±8.9 hours. The patients experienced 14.9±9.6 headaches per month. The associated symptoms observed with headache were nausea in 99 patients (87.6%), vomiting in 31 patients (27.4%), photophobia in 51 patients (45.1%), phonophobia in 20 patients (17.7%), dizziness in 60 patients (53.1%), and visual symptoms in 13 patients (11.5%) (Table 1).
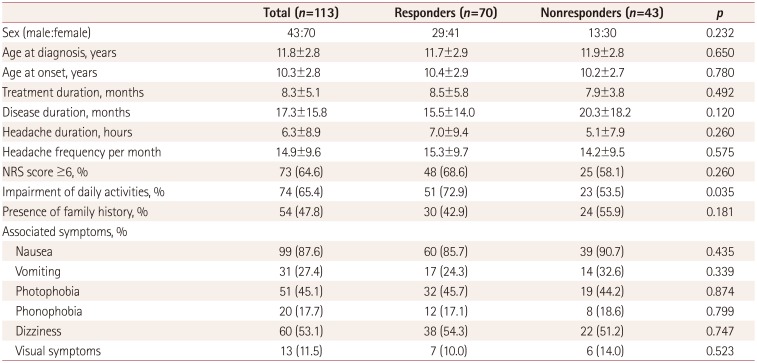
Table 1
Demographics and clinical characteristics as predictive factors of the response to migraine prophylaxis using topiramate
![]()
Seventy patients (61.9%) experienced a reduction in headache frequency of more than 50%. The frequency of headaches decreased from 15.3±9.7 to 1.7±2.8 days per month in the responder group, with no change in the nonresponder group (14.2±9.5 days per month before treatment and 14.2±8.4 days per month after treatment). Sex, age at onset, age at diagnosis, and the duration, intensity, and average monthly frequency of headaches did not differ significantly between the responder and nonresponder groups. The disease duration was longer in the nonresponder group (20.3±18.2 months) before migraine prophylaxis than in the responder group (15.5±14.0 months), but the difference was not statistically significant. The presence of associated symptoms such as nausea, vomiting, photophobia, phonophobia, dizziness, and visual symptoms did not differ between the responder and nonresponder groups (Table 1).
The proportion of patients experiencing significant impairment in daily activities was significantly higher in the responder group than in the nonresponder group (72.9% vs. 53.5%, p=0.035). Family history of migraine was not significantly different between the two groups [nonresponder group (55.9%) and responder group (42.9%)] (Table 1). The results of the ordered logistic regression showed that significant impairment of daily activities was significantly more common in the responder group (p=0.004) (Table 2).
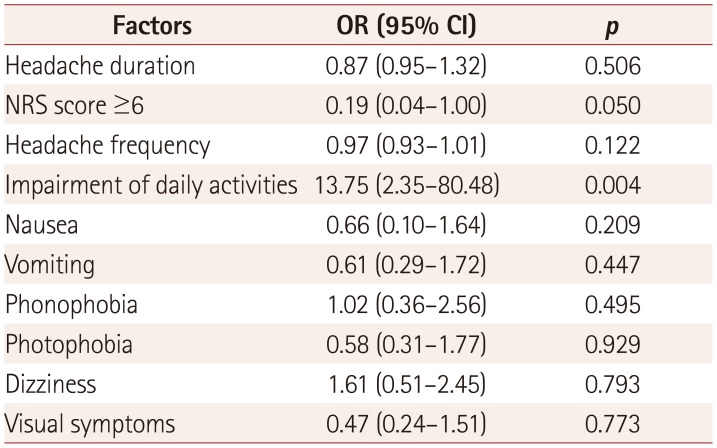
Table 2
Results of ordered logistic regression analysis of predictive factors for topiramate prophylaxis
![]()
Go to :
DISCUSSION
We analyzed demographic features, migraine characteristics, and associated symptoms with the aim of determining if any of these factors were associated with topiramate prophylaxis response in pediatric migraine patients.
The presence of associated symptoms such as nausea, vomiting, photophobia, phonophobia, dizziness, and visual symptoms and the headache duration were not significantly related to the treatment response in our study, which is consistent with previous reports.1920212223 The frequency and intensity of migraines and the presence of a family history were not significantly related to a response to topiramate treatment. The findings of previous studies have been inconsistent. Two studies found that experiencing frequent migraines (more often than eight times per month) led to an unfavorable treatment response (for flunarizine),1921 while other studies found that frequent attacks were associated with better response (for amitriptyline)22 or were no associated with the response (for topiramate and flunarizine).2324 Most studies have found no relationship between headache intensity and treatment response,202122 but one study found a better response when the headache intensity was greater (for flunarizine).19 The presence of a family history was not related to the treatment response in two studies (for amitriptyline and cinnarizine),2022 but one study suggested an association with a positive response (for flunarizine).19 In addition, one study suggested that the treatment response was more unfavorable with a longer disease duration (for cinnarizine).20 Collectively these findings indicate that associated symptoms and headache duration have never been reported to be a predictive factor. The results for the frequency and intensity of migraines and the family history have been conflicting in different studies. However, most studies found no significant relationship with migraine prophylaxis.
Impairment of daily activities was significantly more common in patients who responded well to topiramate prophylaxis. However, a previous study of topiramate prophylaxis in adults utilizing the Migraine Disability Scale (MIDAS) found no significant relationship with the treatment response.23 The main difference between the two studies is that the previous one used a MIDAS score of 61.5 points as a cutoff for defining impairment of daily activities, whereas the present study used subjective reports from patients or caregivers. It is possible to select patients who are expected to show a good response to treatment with a specific drug if the factors underlying the responses are known. This strategy can increase the likelihood of successful treatment and reduce treatment failures. However, the findings of previous studies and the present study indicate the complexity and lack of clarity of the relationship between predictive factors of migraine and response to prophylaxis, with most factors not being related to the treatment response. We also confirmed that migraine characteristics and associated symptoms individually were not related to the treatment response. Patients who experienced severe headaches and had more associated symptoms–and thus experiencing impairment of daily activities–were more common in the responder group. In general, patients with severe headache and many associated symptoms perceive their migraine as being more severe. Therefore, these patients and even their treating physicians may be skeptical about achieving good treatment results. Based on the findings to date, we suggest that topiramate prophylaxis should be actively considered in patients even with severe headaches and associated symptoms. Informing patients about these findings could even improve their treatment compliance.
Characteristics of migraine such as duration and location differ between children and adults.2526 In addition, symptoms associated with migraine experienced by children can differ between different age groups.27 Therefore, applying study results for adult migraine to the pediatric population has limitations. To the best of our knowledge, the present study represents the first attempt to discover predictive factors for a treatment response to topiramate prophylaxis in pediatric patients. We also included dizziness as a migraineassociated symptom, which has often not been considered. Dizziness is experienced by 50–60% of migraine patients, and hence is one of the most common associated symptoms.2829 The prevalence of dizziness in our cohort was 53%. Dizziness is not included in the diagnostic criteria for migraine, and it is difficult to describe objectively, resulting in it being frequently overlooked. There has recently been speculation that dizziness is related to sensory overexcitement symptoms such as photophobia and phonophobia. Future studies should probably include dizziness as one of the key symptoms associated with migraine.30
This study was subject to several limitations. It had a retrospective design and was conducted in a single tertiary center targeting patients treated with topiramate for at least 3 months, which means that the findings might not be applicable to all pediatric migraine patients. In addition, only the associated symptoms included in the diagnostic criteria, dizziness and, visual symptoms were considered. We often observe various symptoms that are concomitant with migraine, such as autonomic symptoms, mood disturbances, cognitive changes, and sensory symptoms.313233 However, these symptoms have never been considered as potential predictive factors due to the limited availability of information about them. Impairment of daily activities can be assessed using the pediatric MIDAS to provide more objective comparisons. In addition, relationships of headache with comorbidities including child abuse, epilepsy, and psychiatric or psychological problems were reported recently,3435363738 but we could not include other comorbidities as predictive factors due to insufficient information and the smallness of the study population. Moreover, confounding factors such as age and the placebo effect may have been present in our study due to the absence of subgroup analysis and a control group. Therefore, a larger prospective study including a broad variety of associated symptoms and comorbidities may be warranted for elucidating predictive factors more precisely.
This study found that migraine characteristics and associated symptoms were not related to the response to topiramate treatment. However, impairment of daily activities was more common in patients exhibiting good responses. Thus, prophylactic treatment with topiramate should be actively considered in patients who experience impairment of daily activities.
Go to :
 XML Download
XML Download