

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal muscular atrophy (SMA) is an autosomal recessive neuromuscular disorder characterized by the degeneration of motor neurons in the spinal cord and brainstem, which results in progressive proximal muscle weakness and atrophy. SMA was first described by Werdnig and Hoffmann.1 The estimated incidence of this disease is 1 in 6,000–10,000 births, with a heterozygous carrier frequency of 1 in 40–60.2
Patients with SMA are classified into the following five subtypes according to the age at onset and clinical severity:3
Type 0 SMA is a prenatal-onset type that manifests as a very severe form.
Type 1 SMA, which is called Werdnig-Hoffman disease, is an infantile type and constitutes 50% of cases. This type mostly presents as floppy infant syndrome, and the patients experience difficulties breathing and feeding.
Type 2 SMA (Dubowitz disease) is an intermediate form showing less-severe symptoms.
Type 3 SMA (Kugelberg-Welander disease) presents after 18 months, and the patients usually maintain the ability to sit and stand.
SMA is known to be caused by mutations in the survival of motor neuron (SMN) gene, which is located on chromosome 5q11.1–13. The telomeric copy of SMN, which is called SMN1, is the disease-determining gene, and about 95% of the affected patients have a homozygous deletion in SMN1.7 In contrast, SMN2, a homologous centromeric copy of SMN1, is considered to be a disease-modifying gene because of the relationship between its copy number and disease severity.8
Another gene, the neuronal apoptosis inhibitory protein (NAIP) gene, which is adjacent to SMN, has been identified as being related to SMA. Previous studies have suggested that patients with a mutation in NAIP show more-severe symptoms, but the direct role of NAIP has not been fully investigated.
The prognosis of SMA is grave, with no curative treatment being available. However, the recent understanding of these representative genes associated with SMA suggests the role of phenotype modifiers and that there is potential for therapeutic intervention. Therefore, we aimed to describe the genotypes and clinical phenotypes of Korean pediatric SMA patients and determine the association between an NAIP deletion and clinical outcomes.
METHODS
A retrospective review of SMA patients treated from July 1999 to July 2013 was conducted at the Asan Medical Center Children's Hospital, University of Ulsan College of Medicine, Seoul, Korea. Thirty-three patients who satisfied the diagnostic criteria defined by the International SMA Consortium9 were included in this study. Demographic characteristics, including the sex, age at symptom onset, and familial history, were obtained from electronic medical records.
On the basis of age at onset and clinical severity, the patients were divided into types 1, 2, and 3. Clinical outcomes were assessed at an outpatient clinic, including the need for ventilator support or death. Laboratory data were obtained, including from electromyography, nerve conduction velocity, serum creatinine kinase, neuroimaging, and muscle biopsy.
Genetic studies to identify deletions in SMN1 and NAIP were performed in all patients. The parents of each patient provided written informed consent. Genomic DNA was extracted from peripheral blood leukocytes using the Puregene DNA isolation kit (Gentra, Minneapolis, MN, USA). The deletion in SMN1 was analyzed according to a previously outlined method,10 being detected by the restriction-fragment-length polymorphism analysis of polymerase chain reaction (PCR)-amplified fragments using the restriction enzymes DraI for exon 7 and DdeI for exon 8. The deletion in the NAIPT gene was detected using multiplex PCR of exons 4 and 5, with exon 12 as a PCR control.11
The clinical characteristics of patients with and without a deletion in NAIP were compared using Fisher's exact test or the Mann-Whitney test. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using the SPSS software package (version 22, SPSS Inc., Chicago, IL, USA).
This study was approved by the Institutional Review Board of the Asan Medical Center (approval no. 2016-0322).
RESULTS
The demographic and clinical characteristics of the patients are listed in Table 1. The 33 patients comprised 12 males and 21 females with a mean age at symptom onset of 14.7 months. Fifteen patients were of type 1, 16 were of type 2, and 2 were of type 3, with mean ages at symptom onset of 3.9, 17.8, and 72 months, respectively. The most common reason for visiting the hospital was respiratory difficulty (49%), followed by hypotonia (30%), gait disturbance (15%), and developmental delay (6%).
The estimation of clinical outcomes was available for 19 patients in medical reviews of visits and calls. Seven of these patients had type 1 SMA, and the other 12 were type 2. Three of the seven type 1 SMA patients died; the characteristics of these patients are listed in Table 2. The four survivors needed ventilator support, and this was started within a year after SMA symptom onset in three of them, and after 2 years in the fourth. Twelve patients with type 2 SMA had no respiratory problems, but all of them needed support from an electric wheelchair or walking aid.
Table 3 presents the results of genetic tests of the patients. Thirty patients (91%) had a homozygous deletion in SMN1 located in exons 7 and 8. Two of the type 2 SMA patients had a deletion in SMN1 in exon 7 only. One type 1 patient had a heterozygous deletion in SMN1, and DNA sequencing of SMN1 showed a homozygous c.836G>T, p.R288M mutation, which was carried by the father of the patient. Six of the 30 patients with the homozygous SMN1 deletion also had a deletion in NAIP.
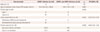
Among the 30 patients with the homozygous SMN1 deletion, clinical variables were compared between those with and without an NAIP deletion (Table 4). All six patients with an NAIP deletion had type 1 SMA. The mean age at symptom onset was lower in those with an NAIP deletion (1.9 months vs. 18.4 months, p=0.007). At the initial evaluation, the patients with an NAIP deletion had more-severe symptoms such as respiratory difficulty or hypotonia [relative risk (RR)=3.33, p=0.003].
Clinical follow-up information was available for 16 of the 30 patients: 4 patients had both SMN1 and NAIP deletions and the other 12 had only an SMN1 deletion. The proportion of patients who had died or received ventilator support was also higher in those with an NAIP deletion (RR=4.68, p=0.009). Among type 1 SMA patients, the presence or absence of an NAIP deletion did not differ significantly with the age at symptom onset (1.9 months vs. 5.5 months, p=0.114) or the initial symptoms (RR=3.00, p=0.198).
DISCUSSION
SMA has been established as the most common cause of death in infants with genetic susceptibility,112 but current treatments are limited to providing supportive care for alleviating the disease burden (e.g., respiratory support and physical therapy). Previous studies have shown that the most severe form (i.e., type 1 SMA) is also the most frequent. The results of the present study are consistent with these findings. Most type 1 SMA patients have poor outcomes with early death or respiratory failure.
Various disease-modifying strategies have recently been proposed following the elucidation of the essential aspects of the pathogenesis of SMA. The SMN protein is one of the key molecules involved in SMA pathology. The full-length SMN protein is considered to function as a chaperone in small nuclear ribonucleoprotein (snRNP) biogenesis and transport snRNPs to the nucleus for RNA splicing.13 SMN1 and SMN2 are inversely duplicated on chromosome 5q13. The telomeric copy (SMN1) produces a full-length SMN protein, while the centromeric copy (SMN2) produces a truncated version of the SMN protein because of alternative splicing.1415 Future therapeutic strategies are aimed at increasing SMN protein levels, either by replacing SMN1 or by splicing modulation or SMN2 activation.4 Although the relationship has not been fully elucidated, the related NAIP is also known to be associated with SMA disease severity.161718
This study has revealed the clinical types and outcomes in Korean pediatric SMA patients and the genotype-phenotype correlation of SMN1 and NAIP deletions. Most (n=30) of the 33 patients were confirmed to have a homozygous deletion in SMN1; the remaining 3 patients had a short heterozygous deletion or point mutation in SMN1. These results are consistent with previous studies finding that most SMA patients had a homozygous SMN1 deletion.7
Several studies have shown that a deletion in NAIP is related to the disease type.161718 Shin et al.19 conducted the first study of deletions in SMN and NAIP in Korean SMA patients; however, NAIP deletions were not detected in any of their five patients. A study of Korean SMA patients that analyzed deletions in candidate genes (i.e., SMN1, NAIP, and p44) did not find a genotype-phenotype correlation, but this could have due to the inclusion of only a small number of patients.20 In a study of Chinese patients, Fang et al.21 compared copy numbers of SMN1, SMN2, and NAIP in SMA patients and healthy controls and produced evidence of differences in copy numbers and gene structure between the SMA patients and controls. Qu et al.22 further investigated the association of copy numbers of SMN2 and NAIP with the disease course in SMA patients, and found that patients with fewer copies of SMN2 and NAIP were characterized by a higher risk of death and a lower survival rate.
Our study included 33 SMA patients, 6 of whom had NAIP deletions and showed a more-severe phenotype of SMA. Moreover, the clinical outcomes of the patients were followed up for a longer duration than in previous studies and showed a clear genotype-phenotype association with an NAIP deletion.
The limitations of our study include the inclusion of a relatively small sample and the lack of an analysis of the SMN2 copy number. However, to the best of our knowledge, this is the first study to demonstrate a correlation between the clinical severity of SMA and SMN1 and NAIP genotypes in Korean patients. Our results imply that an NAIP deletion may serve as an outcome predictor in SMA patients.



 XML Download
XML Download