

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
One significant problem when evaluating patients with cognitive complaints is uncertainty about the accuracy of the information collected during the medical interview. Patients with cognitive impairment may be unaware of or provide minimized reports of their deficits,1 while the personality and effects on the mood of caregivers due to the considerable stress that they may be under might affect their reports.2
Previous studies suggest that reports on cognitive functions obtained from patients are mainly associated with psychological variables, while reports from caregivers are better objective predictors of cognitive impairment.23 Most of these studies have focused on recent memory evaluations and have been performed in the general community or primary care,45 which means that their conclusions might not apply to dementing disorders associated with major executive or language deficits, or to different clinical contexts. Two cross-sectional studies analyzed several cognitive symptoms besides memory complaints, but they were also performed in the community.67
Based on the literature and our clinical experiences, we expected to find significant differences in the meaning and accuracy of cognitive complaints according to their source (patients versus caregivers) and the cognitive area (e.g., memory versus language). We investigated this issue by applying four ordinal scales concerning recent memory, verbal expression, initiative, and mood to both patients and informants, and correlated them with a battery of neuropsychological tests and questionnaires. The ordinal scales allowed us to add a semiquantitative dimension to the answers, instead of merely using “yes or no” questions. The results of this study could provide insight into the meaning of cognitive complaints, and identify which might be better objective predictors of cognitive impairment. In contrast to previous studies, our patients were recruited at a general neurology clinic, which probably included more atypical cases than when recruiting in primary care or the community.
METHODS
The study included a series of patients and informants who were recruited consecutively at the General Neurology Unit of Hospital Ruber Internacional in Madrid, starting in December 2014. We planned a sample size of 74 subjects (37 patients and 37 informants) in order to detect correlation coefficients with absolute values of ≥0.4 with alpha=0.05 and beta=0.02.8 The following inclusion criteria were applied: 1) patients aged 60 years and older who attended the clinic for the first time, 2) a chief complaint of a cognitive or behavioral symptom, 3) available informants, including family members or caregivers in close contact with the patients (personal contact at least 2 days per week), 4) both patients and informants able to complete the ordinal scales, and 5) both patients and informants providing informed consent to participate. In order to reduce selection bias, we did not exclude any patient according to his or her past medical or psychiatric history. The study followed the ethical requirements of our institution and the principles of the Declaration of Helsinki.
We registered the following demographic and clinical variables for the patients: age, sex, education (categorized into four levels: 1) none to preprimary, 2) primary, 3) secondary, and 4) bachelor's to higher), and final clinical diagnosis (obtained after a workup by the attending physician and without pathological confirmation). We also registered the degree of kinship between patients and informants, and the age and sex of the informants.
The respondents provided answers using four ordinal (Likert-like) scales during an interview, which was performed before the neurological examination. These scales consisted of the numbers 1 to 7 equally spaced along a 10-cm-long horizontal line. We used scales with seven categories since this number of divisions seems to provide optimal psychometric features.8 Patients and informants were instructed to mark the numbers that best described the functioning of the patients in four areas: recent memory, verbal expression, initiative, and mood. Lower scores represented worse performance in the corresponding areas.
The neuropsychological tests were administered by a certified neuropsychologist (A.D.B.), who was blinded to results on the ordinal scales. The battery included the Miniexamen Cognoscitivo (a Spanish version of the Mini Mental State Examination, with a maximum score of 35),9 the selective reminding test and the clock test versions included in the 7-Minute Battery,10 categorical (animals) and phonological fluency (letter p) tests,11 the Trail-Making Test (TMT) parts A and B,12 and the 15-item Geriatric Depression Scale (GDS-15).13 The selective reminding test was coded into four variables: naming, free recall, facilitated recall, and recovery [= facilitated recall/(16-free recall), where 16 is the total number of items]. The TMT results were categorized into seven levels based on percentiles in order to apply the normative values of Tombaugh.12 The evaluation also included applying another two questionnaires to the informants: the Shortened Spanish-Informant Questionnaire on Cognitive Decline in the Elderly (SS-IQCODE)14 and the Functional Activities Questionnaire (FAQ).15
Statistical analyses were performed using SPSS (version 20, IBM SPSS Statistics, Armonk, NY, USA). Q-Q plots showed that most of the quantitative variables did not conform to a normal distribution. The correlations between the scores on the neuropsychological tests and the ordinal scales were evaluated with Kendall's tau b coefficient, which was used because it does not depend on the distribution of the variables, and it also allows for ties. We considered p values of < 0.05 in the individual tests to be indicative of statistical significance, but we also estimated p values after correcting for multiple testing using the method of Holm (p Holm). As secondary analyses, we also calculated the correlations separately in demented and nondemented patients; however, the results of these tests should be taken as merely orientative, since the adequacy of the statistical power of the study was based on the entire sample.
RESULTS
The study population consisted of the planned 37 patients and 37 informants, who were recruited within 5 months. Eight other patients were not included because they did not conform with the required criteria: one patient could not complete the scales due to severe aphasia, five patients did not have available informants, and two patients refused to participate.
The patients were aged 75.0±16.6 years (mean±SD), and 20 (54.1%) of them were female. The percentages of patients with education at levels 1–4 were 10.8, 8.1, 32.4, and 48.6%, respectively. Their final clinical diagnoses were as follows (median age, interquartile range; proportion of females): 13 subjects with probable Alzheimer's disease (80.5, 13.7; 54%), 6 with probable frontotemporal lobar degeneration (78.2, 5.8; 83%), 3 with probable Lewy-body dementia (79.0, 6.0; 33%), 3 with vascular dementia (83.9, 2.3; 33%), 4 with amnestic mild cognitive impairment (80.0, 0.8; 75%), 4 with nonamnestic mild cognitive impairment (77.6, 2.0; 50%), 1 with major depression (a 81.2-year-old female), and 3 with subjective memory impairment (66.2, 5.1; 66%). Comparative analyses of demented (n=25) versus nondemented (n=12) subgroups did not show significant differences in age (t=-0.983, df=24.0, p=0.336), sex (Fisher's exact test, p=0.999), or level of education (Fisher's exact test, p=0.265). The informants were all family members (13 spouses, 9 sons, 12 daughters, 1 sister, and 1 grandson) with the exception of 1 unrelated caregiver. They were aged 58.6c8.2 years, and 22 (59.5%) of them were female.
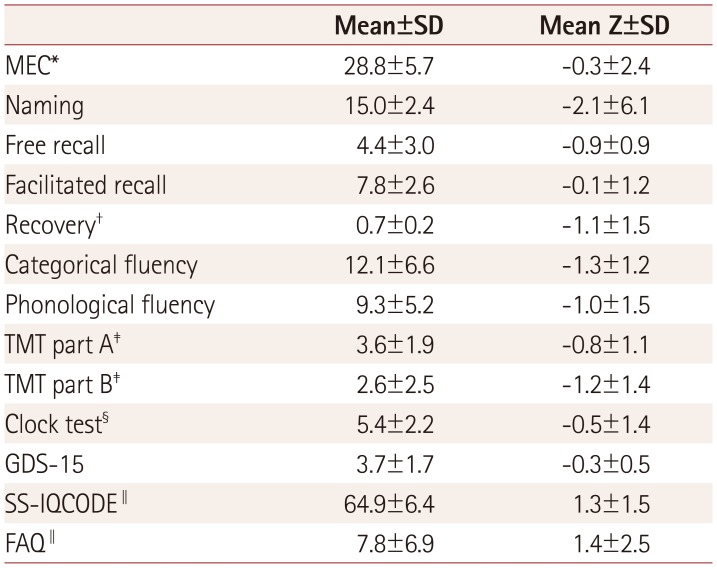
The results of the neuropsychological tests of the patients (n=37) are summarized in Table 1. The scores for the patients (n=37) on the 7-point ordinal scales were 4.9±1.6, 5.2± 1.7, 5.3±1.5, and 5.4±1.5 for memory, verbal expression, initiative, and mood, respectively; the corresponding scores for the informants (n=37) were 3.8±1.4, 4.8±1.6, 4.0±1.6, and 4.8±1.5.
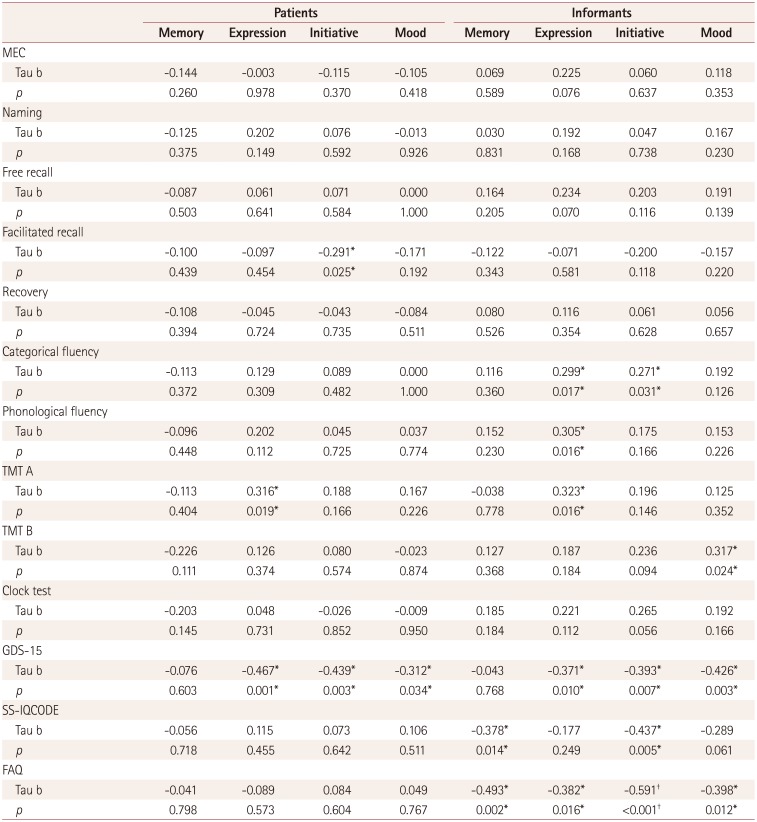
The correlations between the scores on the ordinal scales for patients and informants, and those in the neuropsychological tests and questionnaires are presented in Table 2. The scales from patients were most strongly correlated with GDS-15. There were also weak but significant correlations between the verbal expression scale for patients and TMT part A, and between the initiative scale and facilitated recall. The scores for informants were most strongly correlated with scores on GDS-15, SS-IQCODE, and FAQ. The correlation between the initiative scale from informants and FAQ remained significant after correcting for multiple testing (p Holm=0.013). We also found significant correlations between scores on the verbal expression scale for patients and their phonological fluency, categorical fluency, and TMT part A findings.
Secondary analyses of demented (n=25) and nondemented (n=12) subgroups revealed a similar pattern to that found for the entire sample, although (as expected) the statistical significance of the findings was weaker due to the sample being smaller. Concerning the scales from patients with dementia, the tau b coefficients were highest for the memory scale versus TMT part B (tau b=−0.656, p=0.002), and for the expression (tau b=−0.387, p=0.176) and initiative (tau b=−0.319, p=0.103) scales versus GDS-15. The most significant correlations for the informant scales in this subgroup (demented) were for the initiative scale versus GDS-15 (tau b=−0.574, p=0.055), SS-IQCODE (tau b=−0.410, p=0.040), and FAQ (tau b=−0.512, p=0.007), and for the mood scale versus GDS-15 (tau b=−0.521, p=0.058) and FAQ (tau b=−0.388, p=0.044). The tau b coefficients for nondemented patients were highest for the expression scale versus GDS-15 (tau b=−0.866, p=0.006), the initiative scale versus GDS-15 (tau b=−0.640, p=0.058), and the mood scale versus GDS-15 (tau b=−0.800, p=0.031). The most significant correlations for the informant scales in the nondemented subgroup were for the memory scale versus FAQ (tau b=−0.849, p=0.025) and the initiative scale versus GDS-15 (tau b=−0.552, p=0.152), SS-IQCODE (tau b=−0.583, p=0.042), and FAQ (tau b=−0.667, p=0.033).
DISCUSSION
This study has shown that the meaning and accuracy of the subjective information on cognitive functions obtained in a general neurology clinic vary according to the source (patients or informants) and the area of inquiry (recent memory, verbal expression, initiative, or mood). Subjective information from patients is most strongly correlated with their mood, as estimated using a depression scale (GDS-15), while subjective reports from informants, especially on initiative, are most strongly correlated with the function (as measured using FAQ) and mood of the patients. The information on verbal expression from caregivers was also correlated with both categorical and phonological fluency.
Previous studies on subjective memory complaints (SMC) have not produced consistent conclusions. Several cross-sectional studies found a significant association between SMC and mood, and a weak or no association between SMC and current cognitive performance.5 These findings have been observed in community surveys,21617181920 primary care,21 and memory clinics.22 In contrast, other authors detected significant associations between SMC and formal cognitive tests, particularly in patients with mild cognitive impairment.2324252627 A meta-analysis of the clinical relevance of SMC concluded that they may be useful, when absent, for ruling out dementia or mild cognitive impairment.4 Cohort studies suggest that SMC are predictive of subsequent cognitive impairment,2829303132 but this also has not been a consistent finding.33 Discrepancies between studies might be due to differences in the study populations, the study designs, how SMC are defined, the applied neuropsychological tests, and the analysis methods. Our results on cognitive complaints from patients do agree with most cross-sectional studies, showing a significant association of cognitive complaints from patients and mood, but no or only a marginal association with the findings of formal neuropsychological tests.
The studies referred to above focused mainly on recent memory evaluation. While this may be a reasonable approach in community surveys and primary care, their conclusions might not apply to settings with a significant proportion of patients having dementias other than Alzheimer's disease, such as encountered in neurology clinics. This prompted us to add two questions on verbal expression and initiative. The corresponding scores from patients again showed a significant correlation with mood, and no correlation with the findings of formal cognitive tests, reflecting the pervasive effect of the affective state of patients on their cognitive complaints. A previous cross-sectional study involving community-dwelling older adults produced comparable conclusions.7 In that study, participants and informants were asked a series of questions on subjective cognitive complaints (SCC). SCC were correlated with measures of depression and anxiety, and a statistical analysis showed that psychological factors explained the number of complaints better than the cognitive performance. In contrast, two studies showed significant associations between SCC and objective cognitive performance,634 even after controlling for affective symptoms.6
Classic studies have found that reports from informants are quite accurate for detecting cognitive impairment, but they are also affected by the mood of both the patients and informants.235 In a 10-year study of community dwellers, Watson et al.36 instead found poor concordance between clinical diagnoses of dementia or cognitive impairment and the recognition of memory loss by informants. We found a significant correlation between the cognitive reports from informants and the mood of patients. However, we found an even stronger correlation with the findings of FAQ, which is a functional measure of the instrumental activities of daily life.15 Of particular note is that the correlation between the initiative scale from informants and the FAQ was the only one that remained significant after correcting for multiple testing. This finding suggests that the initiative score could be useful as a surrogate marker of the general functional ability of patients. Finally, we also found a significant association between the score on the verbal expression scale for relatives, and phonological and categorical fluency. Together these data suggest that informants can detect functional and language problems more accurately than memory deficits.
This study was subject to three main limitations. First, it was powered to detect correlation coefficients of 0.4 or higher in the entire cohort, but not in specific demographic (e.g., males versus females) or nosological (e.g., Alzheimer's disease) subsets of interest. Second, SCC were evaluated using four ordinal Likert-like scales due to the lack of uniformly accepted tools for this purpose. Such scales have been shown to be useful for evaluating other subjective symptoms, such as pain,37 and the obtained scores can be readily analyzed using standard statistical tests. Third, the correlations were applied to crude scores that were not adjusted for the level of education. However, the sample was quite homogeneous for this variable, as indicated by the absence of a significant difference between demented and nondemented patients.
In conclusion, the present findings show that cognitive complaints from patients are most strongly correlated with their mood, whilst the reports of informants are most strongly correlated with the functional ability and mood of the patients. When patients themselves complain of problems with verbal expression or initiative, the possibility of underlying depression should be assessed carefully. When asking caregivers about patients, it could be particularly useful to question about initiative, since this seems to be a good marker of general functional ability.
 XML Download
XML Download