

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Carpal tunnel syndrome (CTS) is a common clinical condition caused by entrapment of the median nerve (MN) at the flexor retinaculum of the wrist. Various factors including repetitive wrist movements, obesity, hypothyroidism, pregnancy, diabetes mellitus (DM), and rheumatoid arthritis are considered to be risk factors for CTS.123
Several studies have examined whether DM influences the development of CTS,456 but their results have been inconsistent. The pathomechanism underlying how DM affects the MN is unclear. Furthermore, the exact cause and pathogenesis of CTS are still unclear,7 and the nature of diabetic neuropathy is also controversial since it might be axonal and/or demyelinating. 8 In addition, most studies have performed statistical analyses that did not consider important covariates such as the side of the hand.910 Although DM might systemically affect the peripheral nervous system, it is uncertain how much DM influences focal peripheral neuropathies such as CTS.
A nerve conduction study (NCS) is one of the most sensitive and specific tools for diagnosing CTS,11 and is therefore widely used. However, the NCS criteria for discriminating CTS from other disorders of the MN have not been standardized. Moreover, the severity of symptoms is not always correlated with NCS findings.12 Ultrasonography (US) cross-sectional area (CSA) measurement of the MN has recently been suggested as a complementary method for diagnosing CTS.13 However, previous studies that have used US to investigate CTS in patients with DM did not consider the effect of diffuse polyneuropathy on CTS.1415
We performed this study with the aim of determining the relationship between DM and CTS. We used US CSA as a variable in addition to NCSs to investigate both electrophysiologic and morphologic changes of the MN in patients with DM.1316 We applied a strict statistical design in order to minimize the effects of confounding factors.
METHODS
Subjects
We searched a prospectively recruited neuromuscular US database of a university-affiliated neurology clinic to identify patients who had undergone NCSs and electromyography (EMG) in an upper extremity or in both upper and lower extremities for localized sensory disturbance in the palm of the lateral hand between April 2013 and June 2016. A thorough medical record review was applied to exclude patients with any medical conditions other than DM that could cause peripheral neuropathy. The exclusion criteria also included a history consistent with any cervical spine-related problem, muscle disease, neuromuscular junction disorder, or chronic alcohol intake.
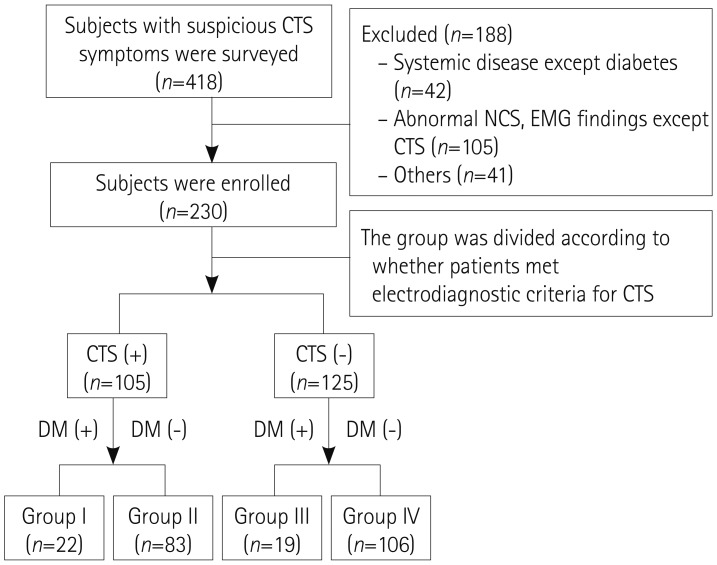
The NCS and EMG results were reviewed to exclude patients who had any abnormal findings except CTS. The patients were then subdivided into two subgroups: 1) those who met the electrodiagnostic criteria for CTS17 and 2) those who had NCS and EMG values within the normal ranges. Only patients with CTS in both hands were included in order to make the statistical analysis more rigorous. The two patient groups were further subgrouped into the following four groups according to the medical history of DM as diagnosed based on the current diagnostic criteria:18 Group I, CTS with DM; Group II, CTS without DM; Group III, no CTS with DM; and Group IV, no CTS without DM (Fig. 1). Demographic data such as age, sex, height, weight, body mass index (BMI), and blood glucose level were collected at the time of the study. The Institutional Review Board of our institution approved the study protocol.
Electrophysiology study
NCSs and EMG were performed using standard electrodiagnostic equipment (Viking IV, Nicolet Biomedical, Madison, WI, USA). The preparation of all patients and all equipment settings and stimulations followed standard protocols.192021 The findings of NCSs and EMG performed on four muscles in each extremity were reviewed.
Only data of the MN from the NCS were used in this study. The MN motor study was performed with stimulation at the wrist, antecubital fossa, and axilla, with recording at the abductor pollicis brevis. The onset latency, amplitude of the compound muscle action potential (CMAP), and conduction velocity (CV) were collected. Using the orthodromic method, sensory studies were performed for the amplitude of the sensory-nerve action potential (SNAP), peak latency, and CV. If the MN sensory NCS results were normal, a comparison test was performed to compare the sensory conduction values of the MN and ulnar nerve (UN) between the wrist and ring fingers. The MN and UN were stimulated at the ring finger using a ring electrode and recorded at 14 cm from the ring finger at the wrist. Differences between the MN and UN latencies of ≥0.5 ms were considered abnormal.22 CTS was classified into six grades based on a Canterbury electrophysiologic grading scale.17
US study
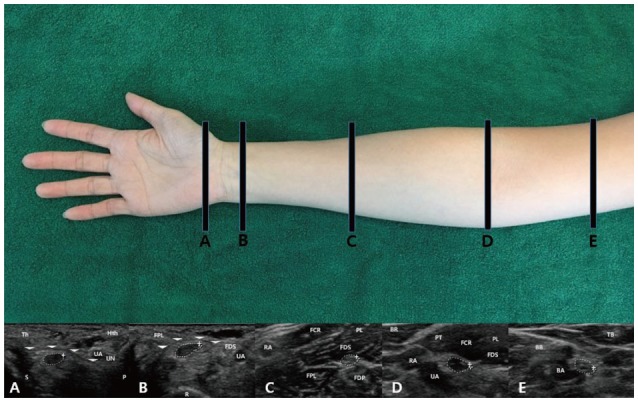
US was performed bilaterally using a 5–12 MHz linear array transducer (HD15 system, Philips Ultrasound, Bothell, WA, USA). The US evaluations followed a previously described methodology.2324 CSA values of the MN were measured at the following five points with anatomical or clinical significance considering the location of the stimulation points in NCSs: location A, the mid-flexor retinaculum (outlet of the carpal tunnel); location B, the proximal flexor retinaculum (inlet of the carpal tunnel); location C, the mid-forearm; location D, the antecubital fossa; and location E, the mid-portion of the upper arm. US tests were performed by tracing nerves from the distal to the proximal region. The CSA at the relevant point of each nerve was measured by manually tracing just inside the hyperechoic rim of the nerve (Fig. 2).
Statistical analyses
Continuous variables are reported as mean±standard deviation and median values, and categorical values are reported as counts (percentages). The Kolmogorov-Smirnov test showed that none of the continuous variables except for the CMAP amplitude and the SNAP CV of the MN conformed to a normal distribution.
In univariate analyses, Kruskal-Wallis tests were used to evaluate the significance of mean differences in CSA values and NCS parameters between the four groups. Mann-Whitney tests were also used for multiple comparisons between groups with Bonferroni correction, with p<0.0083 (=0.05/6) considered indicative of statistical significance. Pearson's chi-square test was used to analyze associations between pairs of categorical variables.
Dependent variables were measured repeatedly on the right- and left-hand sides for all participants. We fitted general linear mixed models with unstructured covariance structures for all dependent variables except the MN CMAP amplitude to determine whether the effects of groups were statistically significant after adjusting for the effects of covariates such as sex, age, side (left and right), location of US, site of the NCS, and group (Groups I, II, III, and IV), and for sex×site, sex×side, site×side, and site×group. We fitted a general linear mixed model with an autoregressive (order-1) covariance structure for the MN CMAP amplitude in the same way.
Probability values with Bonferroni correction were used for multiple comparisons. When we fitted the general linear mixed models, a natural-logarithm transformation was applied to the dependent variables except for the MN CMAP amplitude and MN SNAP CV to improve that fit of the data to a normal distribution.
Statistical analyses were performed using IBM SPSS Statistics for Windows (version 22.0, IBM, Armonk, NY, USA), MedCalc for Windows (version 16.4, MedCalc Software, Ostend, Belgium), and SAS (version 9.4, SAS Institute, Cary, NC, USA). p<0.05 was considered statistically significant (except with Bonferroni correction), and p<0.1 was considered to indicate a tendency that was marginally significant.
RESULTS
Subject characteristics
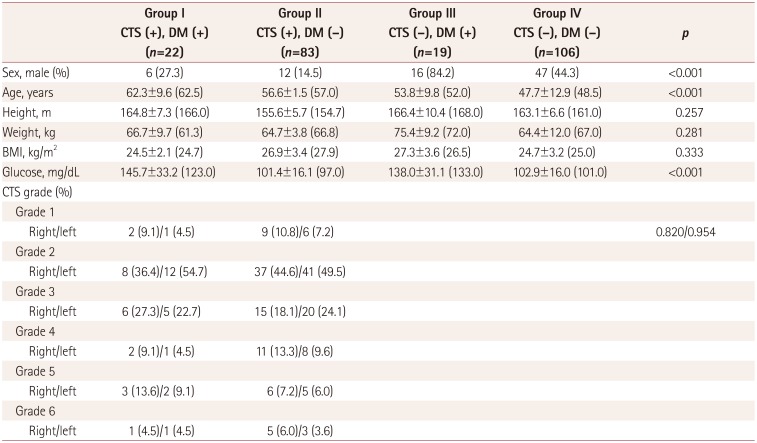
In total, 230 patients were finally selected for analysis and assigned to the 4 study groups as follows: 22 in Group I, 83 in Group II, 19 in Group III, and 106 in Group IV. The proportion of patients with CTS was 53.7% (22/41) in the two groups with DM (Groups I and III) versus 43.9% (83/189) in the two groups without DM (Groups II and IV). The proportion of males was higher in Groups III and IV (without CTS) than in the two groups with CTS. The median age also differed significantly among the four groups. The demographic characteristics of the four groups are presented in Table 1.
US data
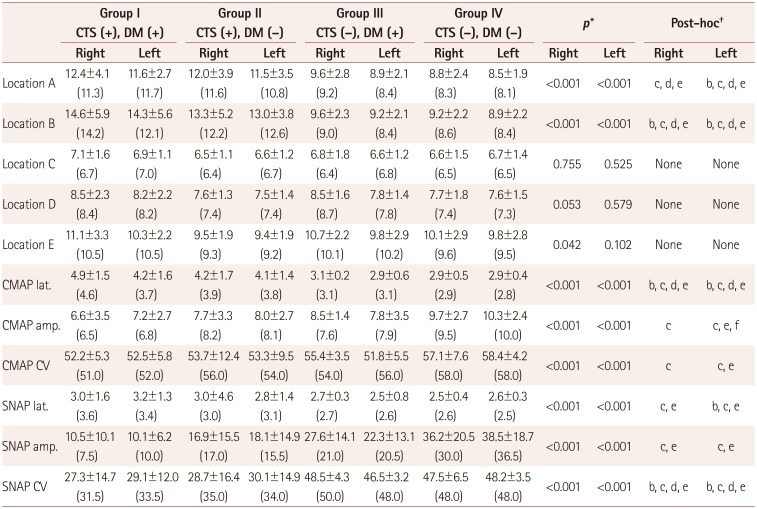
CSA values of the MN measured at each location for the four groups and the results of univariate analyses are listed in Table 2. In pairwise comparisons, the median CSA values at the outlet (location A) and inlet (location B) of the carpal tunnel in both wrists were significantly larger in Groups I and II than in Group IV (p<0.001). These CSA values were also significantly larger in Group II than Group III (p<0.001) and significantly larger in Group I than in Group III (p=0.002) at location B. However, the median CSA values did not differ significantly between Groups I and II at any location, between Groups III and IV at locations A and B, or between any of the groups for the MN at locations C, D, and E.
Comparison of NCS results
Descriptive statistics of the results of univariate analyses of NCS data for the MN on both sides are provided in Table 2. There were marginally significant differences in several NCS values. The right MN CMAP CV and the SNAP latency tended to be lower and longer, respectively, in Group I than Group II (p<0.1). The left MN amplitude and the CV of CMAP also tended to be smaller and lower in Group III than Group IV.
Multivariate comparison of US and electrophysiology data
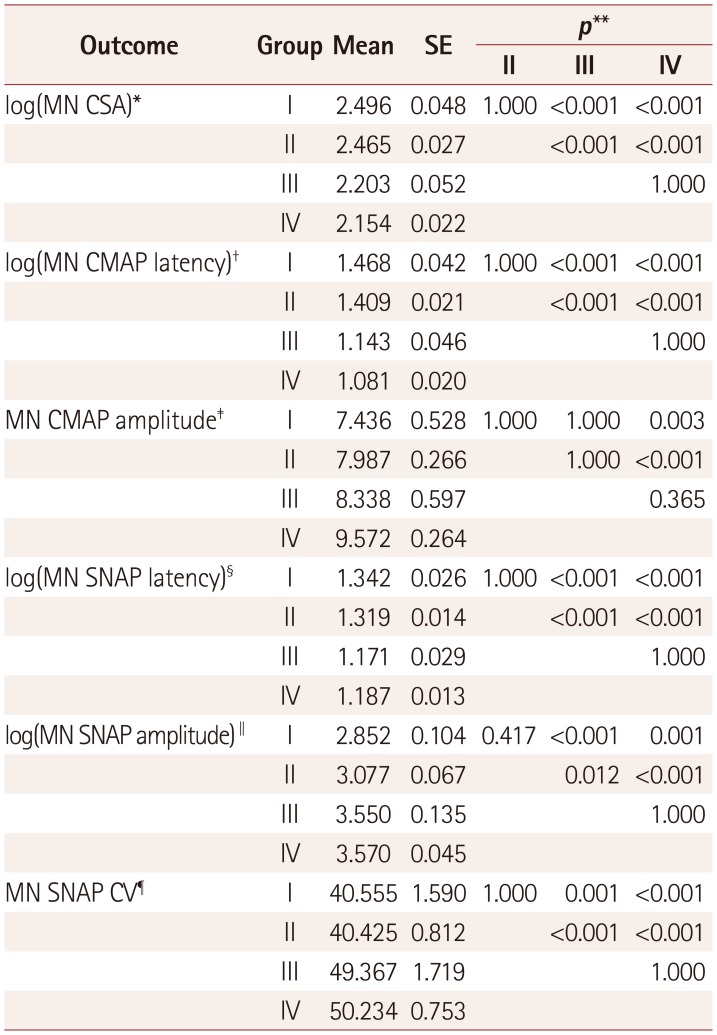
Table 3 presents the results of multiple comparisons of mean values among groups obtained by fitting general linear mixed models adjusted for statistically significant covariates. There were significant differences among the following covariates: sex, group, age, and location in the model for log(MN CSA); and sex, site, side, age, group, sex×site, sex×side, site×group, and side×group in the model for MN SNAP CV.
The mean difference in the estimated log(MN CSA) was 0.293 between Groups I and III (p<0.001), 0.342 between Groups I and IV (p<0.001), 0.262 between Groups II and III (p<0.001), and 0.311 between Groups II and IV (p<0.001). The mean difference in the estimated log(MN CSA) was calculated by subtracting the mean of the estimated CSA for Group III from the mean for Group I, which yielded exp(0.293)=1.34; this value represents the actual CSA difference between Groups I and III. The mean difference in the estimated log(MN CSA) did not differ significantly between Groups I and II or between Groups III and IV.
The mean difference in the estimated log(MN CMAP latency) was 0.325 between Groups I and III (p<0.001), 0.387 between Groups I and IV (p<0.001), 0.266 between Groups II and III (p<0.001), and 0.328 between Groups II and IV (p<0.001). Pairwise comparisons of log(MN SNAP latency) and MN SNAP CV were similar to pairwise comparisons of log(MN CSA) and log(MN SNAP latency). The mean difference in the estimated MN CMAP amplitude was only significant for Groups I and II compared to Group IV.
The only significant difference in the estimated mean difference for log(MN SNAP amplitude) was between females in Groups I and II after fitting a general linear mixed model (p<0.001).
DISCUSSION
Multivariate analysis revealed that the MN SNAP amplitude in NCSs of females was the only variable significantly associated with DM (p<0.001). Groups with DM tended to have a longer latency, smaller amplitude, and a lower CV compared to groups without DM, but these differences were only marginally significant (p<0.1). The measured US CSA values did not differ between groups with and without DM except at sites related to CTS.
Many studies have investigated the relationship between DM and CTS based on the assumption that DM makes peripheral nerves susceptible to entrapment.2526 A population-based cohort study revealed that the prevalence of CTS was higher in patients with diabetes.7 A meta-analysis found DM to be one of the risk factors for CTS.27 In contrast, a retrospective case–control study found that type-2 DM was not associated with CTS in multivariate analyses after adjusting for sex, age, and BMI.28 A similar case–control study suggested that being female, obese, and older were independent risk factors for CTS, but that DM was not significantly associated with CTS.29 A study involving a Dutch population with matched age and sex groups also did not find a relationship between DM and CTS.1
The discrepancies among studies mean that it remains unclear whether DM is a real risk factor for CTS. These discrepancies may be due to the limitations of using NCSs to diagnose CTS. Although an NCS is one of the most sensitive and specific tools for diagnosing CTS,1130 the severity of symptoms is not always correlated with NCS findings,12 and morphologic changes of the MN that occur in CTS are not well reflected in an NCS. In addition, the exact pathogenic mechanisms underlying CTS and diabetic neuropathy are unclear. Several mechanisms including mechanical compression and microvascular insufficiency have been suggested to cause CTS.631 It is also unclear whether diabetic neuropathy is axonal and/or demyelinating. 832 Another reason for the discrepant findings among previous studies may be that most of them have assigned patients to groups by simply counting the total numbers of hands on both sides or the hand from only one side, without considering the effects of various covariates like in the present study, such as side (left and right), site of the NCS, group, sex×site, sex×side, site×side, and site×group.9101533 This could have introduced errors into the analyses. Lastly, previous studies have investigated CTS without considering whether or not polyneuropathy is superimposed, and so CTS by entrapment and polyneuropathy due to systemic metabolic disturbance were not clearly discriminated in the statistical analyses.
We addressed some of these issues by strictly controlling the group compositions. Subjects with any systemic disease other than DM were excluded. To exclude diabetic polyneuropathy, which may be a confounding variable when analyzing the influence of DM on CTS, only patients with completely normal NCS and EMG results (other than for CTS) were enrolled. Moreover, most previous studies have focused primarily on the relationship between DM and CTS, whereas our study design made it possible to determine the impact of DM in non-CTS patients as well.
We added US data to overcome some of the limitations of the NCS. US is an easily available noninvasive method that can be used to evaluate detailed nerve structures, morphologies, and CSA values. The combination of NCSs and US was previously suggested to increase the accuracy of diagnosing CTS in patients with DM.10 To avoid statistical errors, we considered multiple interactions among covariates to evaluate the isolated effect of DM on CTS. Instead of counting the total number of hands on either side or dividing patients into groups based on hand, we divided groups based on patients taking into account side (left and right) effects as covariates.
This study was subject to several limitations. First, we did not consider prediabetes or the duration of DM, which might be confounding factors for the risk of CTS. Second, the sample was small. However, we decreased bias by selecting subjects using a strict statistical design.
In this study–which applied rigorous statistical analyses to overcome some of the limitations of previous studies–there appeared to be more changes in NCS findings for the MN in DM patients than non-DM patients regardless of the presence or absence of CTS. However, US did not reveal a significant relationship between CTS and DM. Further large-scale studies of US and NCS findings in CTS among diabetic patients are needed for further clarification.
 XML Download
XML Download