

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Parkinson's disease (PD) is a neurodegenerative disease defined mainly by a progressive loss of dopamine-producing substantia nigra cells, and it produces both motor and nonmotor symptoms.1 The worldwide distribution of PD occurrence is uneven, with a crude prevalence rate of 6–328 per 100,000 population in India.23 The risk of developing PD increases with age, and the mean age at onset is approximately 65 years.4
There are various studies suggesting a role of Helicobacter pylori (H. pylori) infections in the development of PD as well as a worse motor function and requirement for increased levodopa dosage.15
H. pylori is a ubiquitous Gram-negative bacterium that infects about half of the world's population and is associated with peptic ulcers.67 The reported prevalence of H. pylori seropositivity in India is 50–77%, and its eradication may impact the morbidity experienced by PD patients.8 However, no supporting data are currently available from the Indian subcontinent. The aim of the present study was to identify the role of H. pylori infection in PD in Indian patients and its effect on anti-PD medication.
METHODS
Study population
We prospectively recruited 36 PD patients over a 3-year period from December 2007 to January 2011 at the department of neurology, Nizam's Institute of Medical Sciences, which is a tertiary-care hospital in South India. The protocol of this study was approved by the Institutional Ethics Committee, and informed consent was obtained from all patients before they entered the study.
Inclusion criteria
The inclusion criteria for PD patients were as follows: PD diagnosed based on United Kingdom Parkinson's Disease Brain Bank Criteria,9 a Hoehn and Yahr score of 2–4 as determined by a movement-disorder specialist, a disease duration of at least 3 years, currently receiving levodopa therapy, and presence of motor fluctuations and normal cognition (Montreal Cognitive Assessment score of >25).
Exclusion criteria
Patients with secondary parkinsonism, Parkinson-plus syndromes, severe cognitive impairment, psychiatric abnormalities, or dysphagia were excluded, as were those with a history of gastric lesions, gastric surgery, prior intake of anti-H. pylori medications anytime during their lifetime, history of antibiotic use during the last 6 months, or use of antacids, H2-receptor antagonists, proton-pump inhibitors, domperidone, prokinetic drugs, or any drug potentially affecting gastrointestinal motility and integrity during the last 2 months.
Data acquisition and assessment
Standardized techniques were adapted for assessing risk factors along with socioeconomic strata.10 Data were collected using face-to-face interviews and in physical and neurological examinations. The Hoehn and Yahr stage11 and motor subset of the Unified Parkinson's Disease Rating Scale (UPDRS)-III12 were used to assess the motor severity of PD. Motor examinations were performed both at the practically defined ‘off’ state (12 hours without drugs) and ‘on’ state (best motor response after ingesting at least 1.5 times the levodopa dose being taken daily; a minimum of 200 mg of levodopa). The time from consuming levodopa to the onset of the ‘on’ time (onset time) was noted. After the levodopa challenge, the duration of the ‘on’ time (‘on’ duration) was noted. The individual levodopa daily dosage was noted and was not changed throughout the study period. The total ‘on’ time over 24 hours (daily ‘on’ time) was calculated by the patient from home diaries filled on the day prior to the visit, because this method has been generally employed in previous studies of motor fluctuations in PD.12
Evaluation of H. pylori by serological examination
Serum IgG antibodies to H. pylori were assessed using an enzyme-linked immunosorbent assay IgG antibody test in all patients. We used the EUROIMMUN kit (EUROIMMUN Co., Luebeck, Germany) for the diagnosis. Based on the current literature indicating that this cut-off value for the test has a sensitivity of 100% and a specificity of 94%, we considered values of >20 and ≤20 relative units per mL as positive and negative, respectively.
Cases and controls
PD patients were further divided into two groups based on IgG assessments: cases comprised PD patients who were H. pylori-IgG positive (H. pylori positive), while controls comprised PD patients who were seronegative for H. pylori-IgG (H. pylori negative).
Outcome measurement
All patients continued receiving their dopaminergic treatment at a constant dosage that was maintained for 3 weeks. H. pylori positive patients additionally received triple therapy with amoxycillin (1 mg twice daily), clarithromycin (500 mg twice daily), and omeprazole (20 mg twice daily) for 2 weeks. All patients were followed up at 3 weeks (i.e., 1 week after completing anti-H. pylori treatment in the H. pylori positive group). UPDRS-III scores in both the ‘on’ and ‘off’ states, the onset time, the ‘on’ duration, and the daily ‘on’ time were measured in all subjects at baseline and after 3 weeks. A gap of 1 week was allowed for assessing the actual effect of H. pylori eradication since antibiotics can modify and occasionally worsen the motor symptoms.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS version 16.0, SPSS Inc., Chicago, IL, USA). Descriptive statistical values (mean±standard deviation) were calculated for various continuous variables. The Mann-Whitney U test was used to assess the differences in various parameters between the H. pylori positive and H. pylori negative groups. The Wilcoxon paired rank-sum test was used to compare the effect of anti-H. pylori treatment on various parameters in the H. pylori positive group. All tests were two sided, and a probability value of p<0.05 was considered statistically significant.
RESULTS
The 10.3±36 PD patients included 19 (52.7%) men, and they were aged 60.0 years, with an age range of 41–75 years. Twenty-one patients (55.5%) were hypertensive, 16 (44.4%) had diabetes, none of them smoked, and 7 (19.4%) consumed alcohol regularly. Two patients had a low socioeconomic status, and the educational status varied. Serological testing revealed H. pylori-IgG positivity in 18 (50%) patients.
Baseline (0 week)
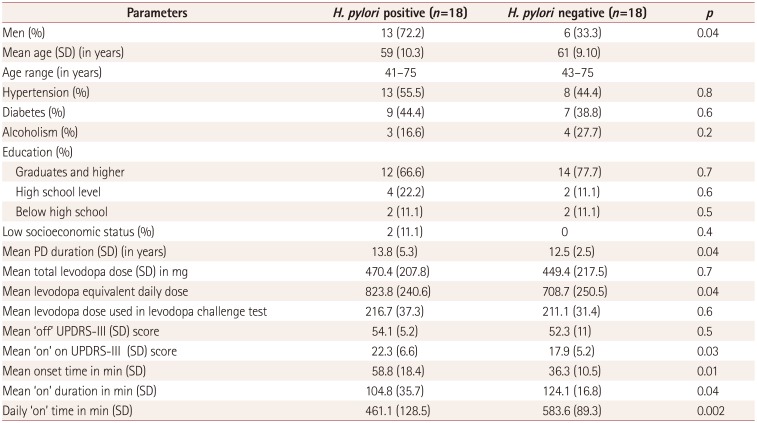
We compared the various parameters at baseline between H. pylori positive and H. pylori negative patients. The prevalence of men was significantly higher among H. pylori positive patients than the controls (72.2% vs. 33.3%), as were the mean disease duration (13.8 years vs. 12.5 years) and the mean levodopa equivalent daily dose (824 mg vs. 709 mg). The levodopa challenge test found no significant difference in the mean levodopa dose between the two groups.
UPDRS-III scores in the ‘off’ state did not differ significantly between the two groups, but the mean UPDRS-III scores in the ‘on’ state were significantly higher and the onset time was significantly longer among patients with H. pylori-IgG positivity, while the ‘on’ duration and daily ‘on’ time were significantly longer among H. pylori negative patients (Table 1).
Follow-up (3 weeks)
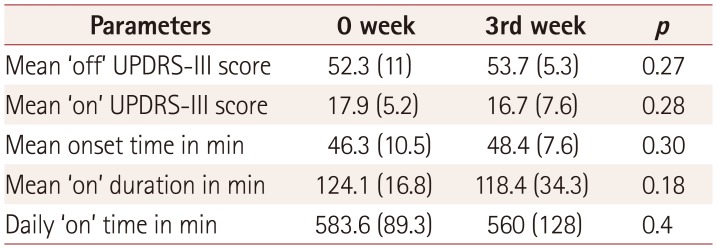
Patients with H. pylori-IgG positivity were assessed before treatment at 0 week and after treatment at 3 weeks. There was significant improvement in UPDRS-III ‘on’ scores, onset time, ‘on’ duration, and daily ‘on’ time after the anti-H. pylori treatment (Table 2). However, there was no significant difference between the various parameters tested at 0 and 3 weeks in the H. pylori negative group (Table 3).
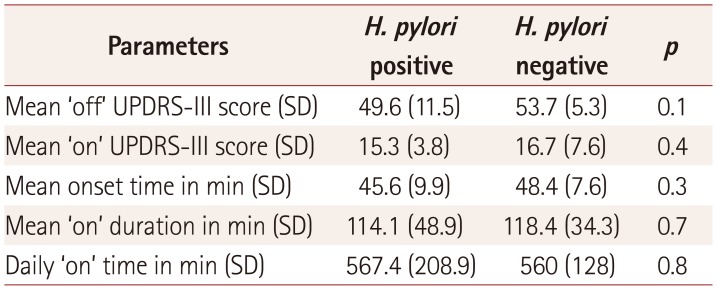
Comparisons of the various parameters between H. pylori-IgG positive patients and controls at the end of 3 weeks revealed no significant intergroup differences in any of the parameters (UPDRS-III ‘off’ and ‘on’ scores, onset time, ‘on’ duration, and daily ‘on’ time) (Table 4).
DISCUSSION
This study found H. pylori-IgG positivity in 50% of PD patients, which is consistent with other studies finding prevalence rates of 40–60% among PD patients.1513141516 The prevalence in our population is also similar to that in the general Indian population.17 Studies from UK and China have shown that the prevalence of H. pylori is higher among PD patients, suggesting a causal role.1819 Schulz et al.20 suggested that H. pylori infection can contribute to the degeneration of dopaminergic neurons by increasing cholesterol glucosides in a manner similar to cycad toxins.
Duration of disease
Our patients with H. pylori infection had a significantly longer disease duration compared to the H. pylori negative patients (p=0.04). A study from Malaysia also found that the prevalence of H. pylori infection was associated with a longer disease duration.5 Poor gastric motility, worsening motor function, poor hygiene, and a growth-promoting effect of levodopa may result in PD patients with a longer disease duration being more prone to H. pylori infection.2122 A bidirectional association of H. pylori infection and PD thus seems to exist, resulting in severe morbidity.
Motor symptoms of PD
Motor symptoms are the most important cause of morbidity among PD patients. UPDRS-III motor scores in the ‘off’ state did not differ between our H. pylori positive and H. pylori negative patients, suggesting similar disease severity. However, the response to levodopa in terms of the time to a response, response duration, and overall response to treatment was worse in the H. pylori positive group than in the H. pylori negative group. These findings are consistent with those of other studies.16
H. pylori infection could affect levodopa absorption via numerous mechanisms.23 It has been demonstrated that H. pylori-related gastritis reduces gastric acid secretion by releasing the proinflammatory cytokine interleukin-1b.23 Levodopa is soluble in an acidic pH and is impaired by alterations in gastric acid. H. pylori also interferes with gastric myoelectric function, leading to gastric immotility and delayed gastric emptying, further reducing levodopa absorption. Other studies have shown that H. pylori may use levodopa for its growth. In vitro studies have shown that H. pylori grows faster in levodopa- and noradrenaline-rich culture media than in media similar to the normal gastric environment. All of these factors may act synergistically to impair intestinal levodopa absorption in vivo. Thus, H. pylori positive PD patients are prone to a poor levodopa response and fluctuations associated with erratic absorption.23
Therapeutic response
H. pylori positive patients were assigned to receive a standard H. pylori eradication treatment, after which there was significant improvement in the response to levodopa. H. pylori negative patients did not receive any eradication treatment and acted as controls, and they showed a similar response to levodopa when assessed after 3 weeks. Our results are similar to those of previously published studies. In a randomized control trial, Bjarnason et al.24 found improvement in gait (stride length, torque-to-flex rigidity, and percentage body sway) among PD patients with H. pylori eradication compared to placebo. Weller et al.25 found that eliminating infection in late parkinsonism can significantly improve motor symptoms and cachexia. Randomized control trials performed in different countries have shown improvements in the motor symptoms of PD (especially motor fluctuations) with H. pylori eradication.151626
These improvements were probably due to improvement in the absorption of levodopa, since the levodopa absorption was found to be increased by 54% after H. pylori eradication therapy.22 We also, found no significant difference between the seropositive and seronegative groups in various disease parameters after 3 weeks. This suggests that H. pylori acts predominantly by impairing levodopa absorption, which is consistent with other findings.23
Limitations of study
This study is the first from the Indian subcontinent, and all patients were evaluated by a single movement-disorder specialist and all laboratory tests were performed at a single laboratory. We have shown that H. pylori seropositivity is common in Indian PD patients and that treatment definitely improves their outcome. However, the present study was subject to a few limitations. It was based on serological tests for detecting antibodies to a specific microorganism, whose presence would indicate that infection with the microorganism occurred at some point in time. Anti-H. pylori antibodies do not always imply the presence of an active infection, and so we may have overtreated our patients. Upper gastrointestinal endoscopy and biopsy as well as rapid urease treatment are suggested for all patients with antibody positivity,27 but most of the PD patients in our clinic refuse this procedure. The urea breath test is a noninvasive technique, but 13C radioactive ligands are not available in our state and serology still remains the most commonly performed test worldwide.28
We applied a combination of amoxycillin, clarithromycin, and omeprazole for 2 weeks to all of the seropositive patients. We were unable to obtain tissue samples for the diagnosis and assessment of antibiotic sensitivity. Worldwide there is an increasing prevalence of resistant strains, although clarithromycin resistance is rare in Indian subjects.2930 Our study had an unblinded open-label design, and hence we cannot exclude a placebo effect. A placebo effect associated with an increase in striatal dopamine in anticipation of a reward can partly contribute to and falsely exaggerate the therapeutic effect in PD.31
Conclusion
This study found a 50% prevalence of H. pylori seropositivity among Indian PD patients and that this population exhibited a worse response to levodopa. The presence of H. pylori infection among PD patients may be missed completely due to the symptoms of dyspepsia and gastric irritation occurring as a nonmotor manifestation of PD or being considered a side effect of levodopa. Erratic absorption of levodopa and motor fluctuations in PD patients can significantly worsen their quality of life, reduce productivity, and increase anxiety and depression. Due to the effect that H. pylori infection has on levodopa function, it is important to recognize and treat this problem in countries where it is highly prevalent. The implication that H. pylori infection may predispose to neurodegeneration and cause PD is still largely unexplored. Large-scale and multicenter studies involving our population may provide an answer in the future.

 XML Download
XML Download