

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The corpus callosum (CC) is the largest brain interhemispheric commissure consisting of white matter. It is therefore involved in many neurologic and systemic pathologies, including congenital diseases, vascular anomalies, and white-matter diseases and tumors.12 Thinning of the CC is well described3 as resulting from either developmental anomalies or injurious diseases, such as ischemia/hypoxia. In contrast, a thickened CC is considered a rare disorder, which is described mainly in fetuses and generally considered an ominous sign at that stage of development.4567 Pashaj et al.8 constructed reference charts for measurements of the fetal CC, but these have been much less established in infants and children. Our experience led us to that a thickened CC is not that rare, and that it is not by itself a sign of an ominous disease.
In the present study we looked at children who were considered to have a thick corpus callosum (TCC) in magnetic resonance imaging (MRI) images, looking specifically for the associated clinical disorders and for potential additional brain malformations. We then measured the CC width in specific regions and compared our findings with the findings for normal CCs, in order to examine the agreement between the observation-based diagnosis of TCC and objective measurements. Our working hypothesis was that for routine clinical purposes, exact measurements of the CC thickness are not superior to observatory clinical evaluations.
METHODS
The hospital Helsinki Committee (IRB) approved the study. MRI images were collected from the archived reports of the weekly neurology/radiology rounds of the hospital pediatric neurology team led by a senior neuroradiologist. The MRI images were reviewed before and during the rounds with the aim of re-evaluating the recorded findings, and the final conclusions of the discussed MRI images were summarized in a dedicated registry. We were able to retrieve the results of the re-evaluated studies as at January 2003. All of the MRI images in which the CCs were considered as being abnormally thick by the senior radiologist were reviewed by considering both clinical observations and comparison with the figures in the article by Suganthy et al.9 to confirm the initial judgement of the abnormality of the CC thickness. Imaging studies in which the CC was considered to be distorted were excluded from the study. The CC was measured in millimeters, and the pertinent clinical data of the children that had led to performing brain MRI were summarized.
The CC was measured in each brain MRI image as described by Suganthy et al.9 A paramedian sagittal section of the brain MRI was selected, and the CC was measured in the following four regions:
1) Anteroposterior length (LC), representing the length of a straight line from the anterior-most to the posterior-most point of the CC.
2) Genu width (WG), representing the distance from the anterior-most point of the CC to the anterior-most point of the inner curvature of the CC.
3) Trunk width (WT), representing the distance between the dorsal and ventral parts at the middle of the CC.
4) Splenium width (WS), representing the perpendicular distance between the ventral and dorsal parts of the splenium at its widest part.
The measurements were performed by A.S. and O.K., and the measured values were analyzed statistically.
RESULTS
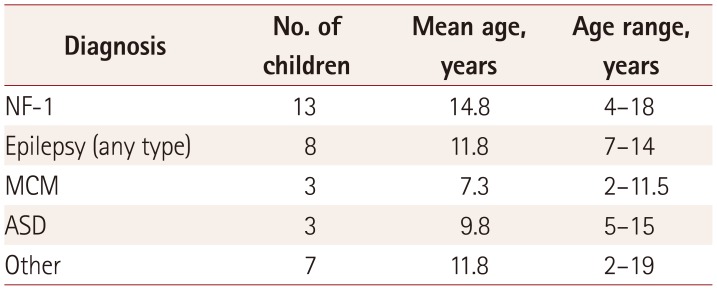
The reports of brain MRI investigations performed during the study period were identified, with TCC being detected in 34 children. Thus, the prevalence of a TCC in this population was 1.3% (Table 1). The average age of these children during the study period was 12.3 years, and 19 were males (54%) and 15 (46%) were females.
Children with neurofibromatosis-1
All 13 children with neurofibromatosis-1 (NF-1) had the typical cutaneous stigmata, and 5 also had ocular Lisch nodules (39%). None of the children was classified as being dysmorphic. All of these children underwent brain MRI as part of the routine workup for their basic disease. They all had NF-1-related hyperintense T2-weighted lesions. The basal ganglia were involved in 12 patients, the brainstem in 10, the cerebellum in 10, and the white matter in 6. Two children had a Chiari-1 malformation. Other findings included enlarged hypophysis, thickened hippocampus, partial arterial circle-of-Willis deficiency, and enlarged ventricles. Three of the children had discrete lesions (unidentified bright objects) inside the CC but without distortion of its contour. Four of the 13 children had coexisting optic glioma (30%), 2 had twisted optic nerves, and 1 had a brainstem glioma. All of the school-aged children attended regular schools, three completed high school, and one was recruited to mandatory military service.
Children with macrocephaly capillary malformation
All three macrocephaly capillary malformation (MCM) children were noted to have developmental delay in addition to macrocephaly, and they attended special education classes. One child was treated with acetazolamide for an increased intracranial pressure. One child had hemihypertrophy of the limbs and another had hepatomegaly. Their brain MRI images all indicated low positioning of the cerebellar tonsils and abnormal periventricular signals in the white matter. Two MCM children had asymmetric ventricles, and two had thickening of the optic nerves.
Children with autistic spectrum disorder
All three autistic spectrum disorder (ASD) children had developmental delay and attended special classes. One child was dysmorphic with microcephaly, and one was macrocephalic with dystonic movements. Dysmorphic pons was detected in MRI of one child. None of these children had a Chiari-1 malformation or low positioning of the cerebellar tonsils.
Children with epilepsy
Of the eight children with epilepsy, one ha Angelman syndrome and another ha acute intermittent porphyria; children was found mentally retarded. The findings of physical examinations of the children was unremarkable, and MRI revealed one child with multiple enlarged perivascular spaces. Seizures in the whole group did not have any unifying characteristic, and no relationship could be delineated between the etiology of the seizures and their semiology. A vagal nerve stimulator was implanted in one child, while all of the others were satisfactorily controlled by antiepileptic medications.
Children with other pathologies
The presence of various etiologies led to neuroimaging being performed in seven children: precocious puberty in two children, growth-hormone deficiency in two children, nonspecific abnormal finding in the neurologic examination in two children, and an increased head circumference in one child. None of these children was mentally retarded. A TCC was the only abnormality in MRI of five children. In one child the cerebellar tonsils were in a borderline position, and another child had cavum septum pellucidum together with a small spinal syrinx.
Measurements
The mean measured values the 4 parameters in the 34 study children were as follows: LC=68.40 mm, WG=11.40 mm, WT=6.37 mm, and WS=17.29 mm (Table 2). There were no significant individual group differences in these measurements, except for LC being significantly lower in the ASD group. There were also no significant gender-based differences for the total cohort or for the individual diagnostic groups. Comparisons of our results with those of other studies in Table 2. In our study, the WG, WT and WS values were higher than the values reported by Suganthy et al.9 (p<0.01 for WT, p<0.01 for WS, and p=0.069 for WG). In addition, the mean LC value in our study was lower than those in the other studies, including those involving children. Measurements in the other selected regions were not available in the other studies.1011
DISCUSSION
In the following study we investigated the frequency of a thick corpus callosum in children, diagnosed by revised observational determination by an experienced neuro-radiologist. This overall frequency was found to be 1.3%.
No specific major neurologic disorder that could be associated with the TCC was detected. It can be suggested that being asymptomatic leads to under-diagnosis of this lesion. Several factors probably also influence its low prevalence. It could be due to the lack of precise criteria to define the corpus callosum as really thick in children or due to relatively low awareness of its existence. Thus, children with a TCC can go undiagnosed or even be misdiagnosed.
In our study, the CC was defined as thick based on judgement of a neuroradiologist. This diagnostic approach can be biased by the radiologists subjective personal characteristics. Nevertheless, it can be presumed it provided a close number, due to the large total number of children, from whom those with thick CC incidence was extrapolated. We should also mention that in some cases different measurement methodologies were found to produce discordant results.12
Out of a total population of 250 children with NF-1 who were being followed at Schneider Children's Medical Center of Israel, 13 had confirmed TCCs on their brain MRI images, yielding an estimated frequency of 5%; this suggests that the prevalence of a TCC is about threefold higher in NF-1 than in the general population. The CC continues to grow until adolescence, after which it is believed to diminish slightly in size.1113 However, our children were unique in exhibiting high WG, WS, and WT values (Table 3), meaning that the CC was very thick.
We were unable to clearly delineate any mechanism underlying the increased thickness of the CC associated with a variety of pathologies that do not have a common pathogenesis. This finding is also known pathologic processes affecting the brain in NF-11415 as well as in MCM,16 but not the pathogeneses of the other conditions our study children. Given that a TCC is rare in epilepsy and is not correlated with any specific pattern of seizures, it is reasonable to consider that the CC, which is composed of white matter, plays no significant role in epileptogenesis. Indeed, the finding of a CC was not associated with specific disorders of the white matter in any members of our pediatric population. Finally, our literature search yielded no description of a CC in ASD patients, but rather evidence of a smaller CC.171819
Contrary to most reports in the literature that claim that a TCC usually involves a grave prognosis, mental retardation, and/or serious developmental delay,202123 our results consistently excluded its specific association with a serious prognosis. Of course, the prognosis in an individual patient is dependent upon the underlying condition with which the thick CC was described, and one cannot infer from our cases that a TCC is a prognosis-determining feature. Nevertheless, most of our study children (mainly in those with NF-1, nonsyndromic epilepsy, and the group of other pathologies attend normal schools and do not suffer from any major disability in their daily life, in direct contrast to another study of an NF-1 population which concluded that an enlarged CC is associated with cognitive impairment.24
We found a relatively high proportion of cases with a Chiari-1 malformation or low positioning of the cerebellar tonsils, i.e., 6 out of 35 children (17%, mainly in the MCM and NF-1 groups), one-half of whom were not macrocephalic.
Lastly, in none of our children an abnormal CC was detected prenatally in routine studies. It in our impression that a TCC may be a TCC a postnatally acquired anomaly. We recommend that the generation of more data on CC measurements to refine our understanding of its involvement in pathologic processes.
In conclusion, it seems that a TCC can be found in children with various diagnoses, especially NF-1 and MCM. We were unable to relate any specific abnormal clinical finding to its existence. However, in some children it was associated with a Chiari-1 malformation. More studies are required to better define this presentation of TCC.


 XML Download
XML Download