

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alzheimer's disease (AD) is a neurodegenerative disease that is the most common type of dementia, the main symptom of which is cognitive decline associated with memory failure. It is unclear how AD will progress, and the clinical symptoms appear later than the disease onset, which makes early diagnosis and intervention difficult.1,2 An earlier diagnosis could help to reduce cognitive deterioration and/or treatment costs. It is also important to understand the disease progression when performing clinical trials.
To overcome these problems, the Alzheimer's Disease Neuroimaging Initiative (ADNI) proposed two stages–early mild cognitive impairment (EMCI) and late mild cognitive impairment (LMCI)–based on the education-adjusted scores of the Wechsler Memory Scale Logical Memory II.3,4 Patients with EMCI and LMCI were subdivided solely on the Logical Memory II score of the Wechsler Memory Scale, but other biomarkers such as the hippocampal volume and cerebrospinal fluid (CSF) biomarkers also showed empirical trajectories suggesting that EMCI could be a transitional stage.5 Thus, understanding differences between EMCI and LMCI might facilitate the understanding of disease progression specifically in mild cognitive impairment (MCI).
Shape-based morphometry has often been applied for analyzing structural changes in subcortical structures, including in the hippocampus.6,7,8,9,10,11,12 Researchers have previously used volumetric analyses for quantitatively assessing hippocampal atrophy as a marker for the progression of AD.13,14 However, changes in volume in certain regions can be compensated for by atrophy or dilation in other locations, which may obscure changes in the total volume. This indicates that volumetric analyses may not reveal the true association between local deformations and the disease or risk factors.12 Additionally, volumetric analyses do not give information about the morphological changes that characterize the appearance and progression of neurodegenerative diseases. A precise analysis of these changes could provide useful early diagnostic information and help to identify individuals at risk.
Early studies using diffusion-tensor imaging (DTI) in AD focused particularly on fractional anisotropy (FA). However, some studies15,16,17 found this measure to be insensitive to early white-matter disruption in AD. Furthermore, most of the relevant studies18,19,20,21,22,23,24 have focused on the changes in large-scale white-matter tracts. This approach is based on the idea that white-matter changes could be the result of Wallerian degeneration, which involves earlier loss of cortical neurons.25,26 Also, clinical abnormalities have been shown to be correlated more strongly with gray-matter changes than with white-matter changes,27 and the presence of cortical gray-matter damage has been demonstrated by diffusion MRI in multiple sclerosis.25
A few studies28,29,30,31,32,33 have investigated microstructural changes within the hippocampus in AD. They demonstrated increased mean diffusivity (MD) in the left hippocampus to be the best predictor of disease progression. However, these analyses relied on manual segmentation of the hippocampus or did not use masking to isolate the hippocampus. This limitation may be attributed to the risk of partial volume effects and the complexity of segmentation.
In the present study we adopted a novel segmentation method that involves subtle volume extraction and better shape reconstruction to input images compared to previous methods.12 We also decomposed the MD into axial diffusivity (AxD) and radial diffusivity (RD) in order to assess the gray-matter abnormalities in EMCI. The overall aim of this study was to characterize the morphometric and microstructure changes in subregions of the hippocampus in EMCI in order to identify the early signature of AD.
METHODS
Demographics
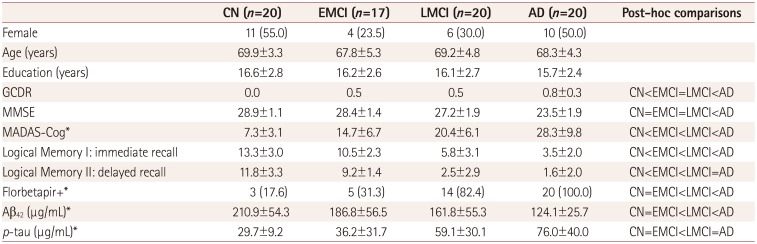
In the phase ADNI2 database, subjects who underwent both T1-weighted and DTI with a visit identifier of “ADNI2 Screening MRI-New Patient” comprised 49 cognitive normal (CN) subjects, and 27 EMCI, 34 LMCI, and 47 AD patients. As an initial study, subjects were sampled with the following criteria: aged 60–75 years, education duration of 12–20 years, and gender matching within groups. Note that the lack of female data for EMCI limited the number of subjects in each group.
The T1-weighted and DTI images of 77 subjects (20 CN, 17 EMCI, 20 LMCI, and 20 AD) were gathered from the ADNI (http://adni.loni.usc.edu). The MRI protocol is described elsewhere.34 We only used the images acquired at the first visit of each subject. The following clinical and neuropsychological assessments were included: global Clinical Dementia Rating, Mini Mental State Examination (MMSE), Modified Alzheimer's Disease Assessment Scale-Cognitive subscale (MADAS-Cog), and Wechsler Memory Scale Logical Memory I & II. Florbetapir PET image data were acquired from the ADNI database with a positivity cutoff of 1.11. The CSF amyloid beta and phosphorylated tau concentrations were measured using the multiplex xMAP Luminex platform. Full details of the analysis can be found online (http://adni.loni.usc.edu/methods/biomarker-analysis/).
The demographics of the included subjects are presented in Table 1. Note that some of the subjects did not undergo a MADAS-Cog assessment, florbetapir PET imaging, or CSF screening, since these interventions are recommended for detailed assessments rather than being applied in routine care settings. Those subjects who did not undergo a MADAS-Cog assessment were excluded from the correlation analysis with clinical scores.
Surface morphometry
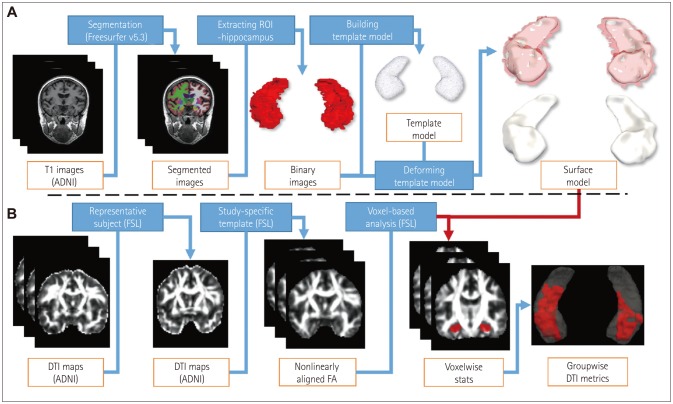
We used progressive template surface deformation to generate a hippocampal template.12 This method involves building the pairwise correspondence of a template surface by minimizing geometric distortion while robustly restoring the shape characteristics of the individual subject. First, we constructed an average template surface of the CN group to use as a region of interest for DTI voxel-based morphometry (VBM) analysis on Montreal Neurological Institute (MNI) 1-mm isotropic space. We then compared T1-weighted MRI hippocampal subfields between the EMCI and LMCI groups (Fig. 1A). Significant dilation was not detected in any region, and so we assumed that the changes in morphometry were due to regional atrophy. All statistical analyses were controlled for age, gender, and years of education. To delineate the surface of the hippocampal subfields, we segmented the average template surface following rules from an anatomy atlas textbook, as described previously.35
DTI analysis
For DTI analysis, the data from an additional 20 AD patients were included to show the characteristics of disease progression. The functional MRI of the brain software library (FSL) Tract-Based Spatial Statistics (TBSS) pipeline was used to construct a study-specific template, and DTI index maps were registered to this template in an MNI space.36 Clusterwise group comparisons of DTI metrics within the hippocampus were performed using the FSL randomise function with the Threshold-Free Cluster Enhancement37 option along 10,000 permutations33 (Fig. 1B). To further analyze the relationship between microstructural integration changes with clinical scores, linear regressions were performed to identify significant clusters. MMSE and MADAS-Cog scores were used for the general clinical assessments. All statistical analyses were controlled for age, gender, and years of educaeducation, and clusters smaller than 100 mm3 were discarded.
RESULTS
Hippocampal volume
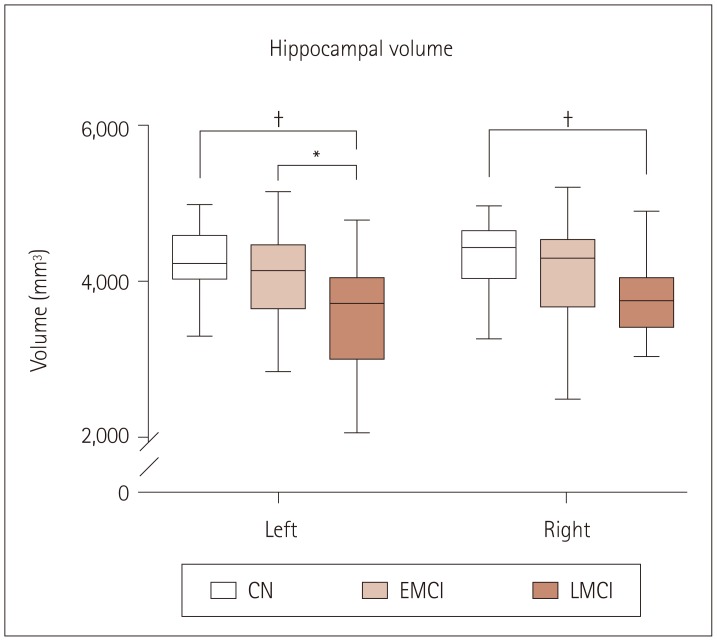
We compared the hippocampal volume using Freesurfer segmentation in each group with regard to laterality. Left hippocampal volumes in EMCI did not differ from those in CN, while those in LMCI were smaller than those in CN (p<0.001) and EMCI (p<0.05). Right hippocampal volumes in EMCI did not differ from those in CN and LMCI. The volumes in LMCI were smaller than those in CN in both hippocampi (p<0.001) and smaller than those in EMCI in the left hippocampus (p<0.05) (Fig. 2).
Hippocampal shape modeling
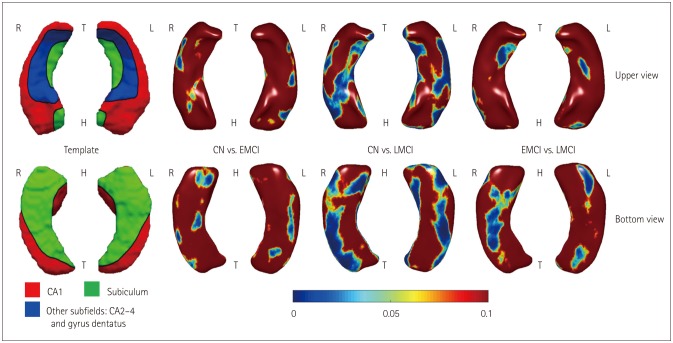
Hippocampal surface analysis revealed significant atrophy in bilateral CA1 regions and the right ventral subiculum in EMCI compared to CN, and in bilateral CA1 and CA2–CA4 regions and the subiculum in LMCI. Direct comparison of EMCI and LMCI revealed that atrophy in the right ventral subiculum part of the hippocampus was more significant in LMCI (uncorrected p<0.05) (Fig. 3).
Hippocampal microstructural changes
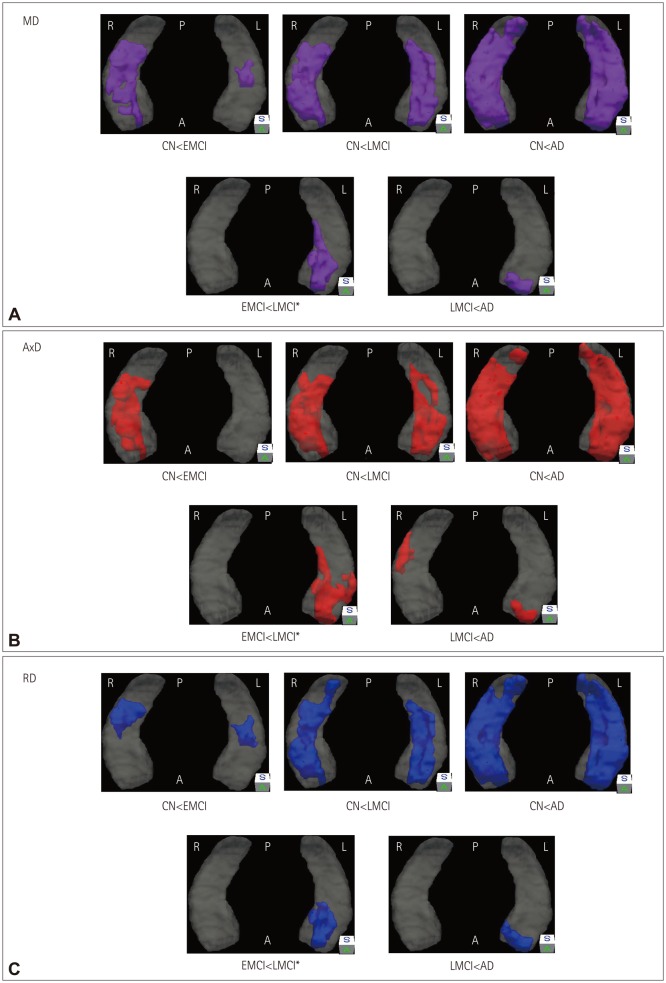
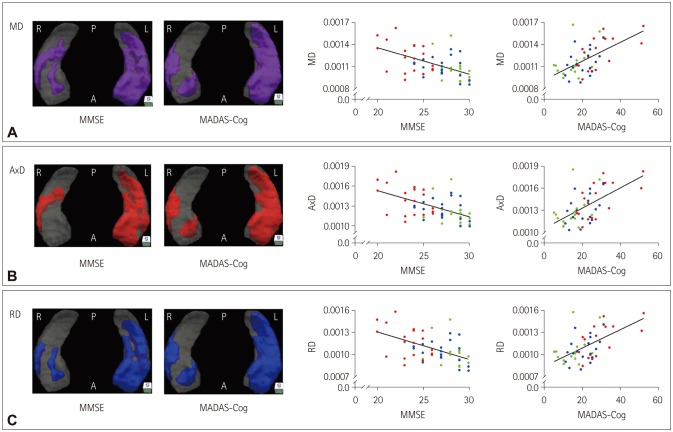
We investigated differences in the diffusion parameters in the gray matter, which reflect microstructural changes. This is not possible via the conventional TBSS approach, which focuses only on white-matter areas, and so we examined voxelwise DTI metrics within the gray matter. The DTI VBM results indicated that the regions of increased DTI metrics grew larger with the disease stage onward (Fig. 4). Note that there were no significant group differences in FA.
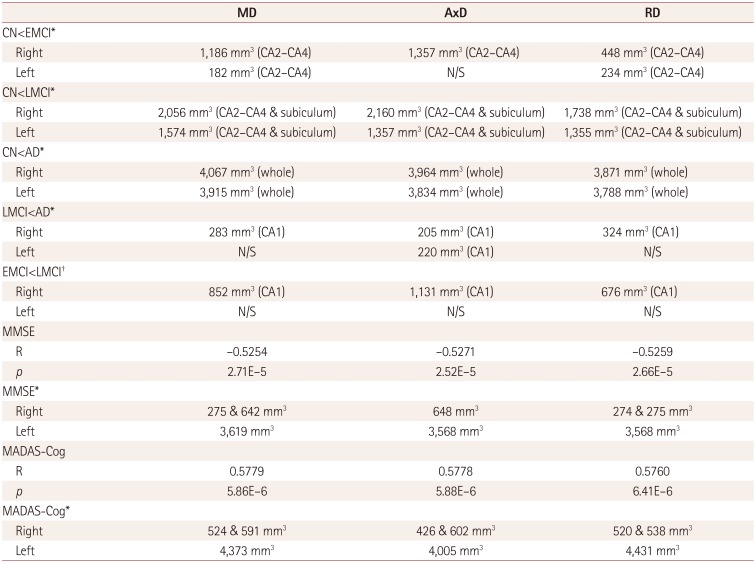
MD was higher in EMCI than in CN in the bilateral CA2–CA4 regions, higher in LMCI than in CN in the bilateral CA2–CA4 and subiculum regions, higher in AD than in CN in most hippocampal regions, and higher in AD than in LMCI in the left hippocampal CA1 region [p<0.05, familywise error (FWE) corrected]. Direct comparison of EMCI and LMCI revealed that the MD was higher in the left hippocampal CA1 region in LMCI (uncorrected p<0.05) (Fig. 4A, Table 2).
AxD was higher in EMCI than in CN in the right CA2–CA4 regions, higher in LMCI than in CN in the bilateral CA2–CA4 and subiculum regions, higher in AD than in CN in most hippocampal regions, and higher in AD than in LMCI in the bilateral CA1 regions (p<0.05, FWE-corrected). Direct comparison of EMCI and LMCI revealed that AxD was higher in the left hippocampal CA1 region in LMCI (uncorrected p<0.05) (Fig. 4B, Table 2).
RD was higher in EMCI than in CN in the bilateral CA2–CA4 regions, higher in LMCI than in CN in the bilateral CA2–CA4 and subiculum regions, higher in AD than in CN in most hippocampal regions, and higher in AD than in LMCI in the left hippocampal CA1 region (p<0.05, FWE-corrected). Direct comparison of EMCI and LMCI revealed that RD was higher in the left hippocampal CA1 region in LMCI (uncorrected p<0.05) (Fig. 4C, Table 2).
Correlations between microstructural changes and clinical scores
Clusters correlated with the MMSE and MADAS-Cog clinical scores were found in the hippocampus in the EMCI, LMCI, and AD groups (Fig. 5, Table 2). The scatter plots in that figure show linear relationships between diffusivity and clinical scores. Note that there was no significant correlation with FA.
MD within the hippocampus showed significant correlations with the MMSE and MADAS-Cog scores (p<0.05, FWE-corrected). Using the mean MD within a cluster to calculate linear relationships yielded R=-0.5254 and p=2.71×10-5 for the MMSE score, and R=0.5779 and p=5.86×10-6 for the MADAS-Cog score (Fig. 5A, Table 2).
AxD within the hippocampus showed significant correlations with the MMSE and MADAS-Cog scores (p<0.05, FWE-corrected). Using the mean AxD within a cluster to calculate linear relationships yielded R=-0.5271 and p=2.52×10-5 for the MMSE score, and R=0.5778 and p=5.88×10-6 for the MADAS-Cog score (Fig. 5B, Table 2).
RD within the hippocampus showed significant correlations with the MMSE and MADAS-Cog scores (p<0.05, FWE-corrected). Using the mean RD within a cluster to calculate linear relationships yielded R=-0.5259 and p=2.66×10-5 for the MMSE score, and R=0.5760 and p=6.41×10-6 for the MADAS-Cog score (Fig. 5C, Table 2).
DISCUSSION
This study aimed to identify the features of EMCI in terms of hippocampal morphology and microstructural changes. As described in the Introduction, we addressed the earlier detection of MCI with respect to structural changes in the hippocampus. While several studies have examined changes in EMCI, significant EMCI-related anomalies are not well documented. Moreover, the present study is the first to reveal both surface deformation and microstructural changes in the hippocampus in EMCI. The findings of this study provide additional knowledge about earlier MCI-related changes in the structure of the hippocampus.
The adoption of progressive template surface deformation made it possible to identify the changes in EMCI that were not detected by conventional volumetric analysis (Figs. 2 and 3). Although we could identify the morphometric changes in EMCI, these were related to disease progression rather than being a characteristic of EMCI. Atrophy in EMCI was present in the hippocampal CA1 region and the right ventral subiculum, which is in accordance with previous reports38,39 of amnestic MCI (aMCI) changes. In addition, the accumulation of neurofibrillary tangles in specific hippocampal subfields and the associated neuronal loss are well documented. The presence of tangles has typically been reported to occur first in the entorhinal cortex, followed by spreading to the subiculum and CA1, then to CA2 and CA3, and finally to CA4.40 A postmortem study of AD brains also found that the subiculum and CA1 were the most affected regions.41,42 These findings confirm that EMCI may predate LMCI in the perspective of AD progression.
LMCI was characterized by a volume decrease in the left hippocampus but additional atrophy relative to EMCI in the right hippocampus (Figs. 2 and 3). A previous study43 found left-less-than-right asymmetry of the hippocampal atrophy as a characteristic change in aMCI. However, one study44 found that right hippocampal changes can occur up to 10 years before the clinical onset of AD. Although that study employed a volumetric analysis, its findings suggest that damage to the right hippocampus characterizes a transition from healthy aging to MCI. This discrepancy could also plausibly be explained based on the characteristics of aMCI patients or differences in difficulties between verbal and visual memory tests. Impairments in verbal memory would presumably be detected more easily by caregivers than those of visual memory. Thus, there is a greater likelihood of including verbal-type aMCI–which would be associated with greater atrophy in the left hippocampus–than visual-type aMCI according to previous studies. As a result, left-right asymmetry of the hippocampus could be collective changes in EMCI and LMCI.
Our DTI analysis also revealed microstructure changes in the hippocampus. DTI is commonly used to measure the large-scale integrity of the white matter. However, there have been recent studies28,29,30,31,32,33 of microstructural changes within the gray matter. In the present study we found progressively larger regions of increased diffusivity during the disease progression, starting from the CA2–CA4 regions in EMCI to the bilateral CA2–CA4 and subiculum regions in LMCI (Fig. 4). While macroscopic changes in EMCI and LMCI showed right hippocampal surface atrophy, microscopic changes were characterized by left hippocampal gray-matter abnormalities. Considering the increased AxD in the right hippocampal CA2–CA4 regions, with mild atrophy in the CA1 region and the subiculum in EMCI, microscopic changes may precede those of surface atrophy. Furthermore, these differences in morphometry and microstructure could represent early changes in MCI. These findings might indicate that microstructural changes such as synaptic loss, neuronal soma changes, and neuronal disorganization occur along with the neuronal loss in the hippocampus.45
Hippocampal asymmetry was also found in the linear relationship between diffusivity and clinical score (Fig. 5), which is consistent with the finding of den Heijer et al.46 The diffusivity in a relatively small area of the right hippocampus was correlated with the clinical scores, and this might be due to earlier gray-matter disruption in the right hippocampus in EMCI. Hippocampal dissociation was previously demonstrated using optogenetics in mice.47 That study showed that optogenetic silencing of either the left or right hippocampal CA3 region impaired the short-term memory, while only left hippocampal CA3 silencing impaired the long-term memory. Considering this dissociation, we suggest that early gray-matter abnormalities in the right hippocampal CA2–CA4 regions in EMCI can cause short-term memory loss while long-term memory in MCI remains intact.
Previous studies28,29,30,31,32,33 have mainly found increased MD within the hippocampal gray matter, along with no AxD changes. An increase in MD is often attributed to the progressive loss of cellular barriers or an increase in extracellular water content, such as occurs during neurodegeneration.48,49,50 However, our findings showed significant overlap between MD and AxD, with a relatively partial overlap between MD and RD. Considering that MD is the combination of AxD and RD, the main difference in MD could be due to AxD changes (Fig. 4, Table 2). A recent study51 found negative correlations between the traverse relaxation rate (R2) and DTI eigenvalues both in vitro and in vivo. R2 is the reciprocal of the transverse relation time (T2) multiplied by 1,000 ms/s. In the presence of damage, this measure decreases as the amount of tissue water increases, which reflects abnormalities in the structural integrity of tissues.51,52,53,54 Rulseh et al.51 found lambda 3 to be the most sensitive index for R2. However, considering RD as a combination of lambda 2 and 3, its sensitivity might be lower than that of lambda 1, which corresponds to AxD. Thus, to explain the elevation of water content as well as tissue damage, AxD could be a better index of neuronal damage within hippocampal gray-matter abnormalities.
This study was subject to several limitations. First, the number of subjects included in the analysis was small in order to observe progressive changes in MCI. As an initial study, we sought to control age, years of education, and gender in the cohort, while targeting subjects who were newly added in the ADNI2 phase in 2014. However, it was difficult to control the gender distribution in the EMCI group. Moreover, it is well known that males show higher diffusion properties than females, which made gender control a crucial factor in this study. We therefore targeted a rather small number of subjects in each group in order to control gender. Second, the initial design of this study did not consider subject inclusion criteria such as AD conversion or positivity for AD biomarkers. In order to focus on progressive changes, potential subjects who may progress to AD should be considered. However, screening was applied only once without follow up in several subjects in this study, or only MRI data were available. Lastly, a longitudinal study involving LMCI convertors from EMCI could better capture the progressive changes in MCI subtypes. Rather than group comparisons of EMCI and LMCI, consecutive changes within the same subjects should be considered in future studies.
In conclusion, we have investigated morphological and microstructural changes of the hippocampal surface in EMCI using structural MRI and DTI. EMCI showed hippocampal surface changes mainly in the CA1 region and the right ventral subiculum, and diffusivity increases in the CA2–CA4 regions. In addition, the diffusivity results showed laterality changes (especially in AxD) in EMCI. These results indicate that certain regions of the right hippocampus are affected earlier than those in the left hippocampus. However, further studies are needed to confirm these laterality changes. We also demonstrate that the diffusivity in the hippocampus is strongly correlated with the cognitive performance, indicating the possibility of using diffusivity as a biomarker for AD progression.
 XML Download
XML Download