

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke is a leading cause of death and disability in Korea, with approximately 105,000 Korean citizens experiencing a new or recurrent stroke annually.1 Environmental factors crucially affect the incidence of stroke, and the meteorological conditions might also significantly influence the seasonal and daily variations of the incidence of stroke. To reduce the burden of stroke, it is crucial to identify modifiable risk factors. However, the association between daily temperature and the incidence of stroke has been largely unknown in Korea.
Several studies have found changes in meteorological parameters and seasonal variation to be associated with stroke worldwide. Most previous studies have focused on the relationship between the incidence of stroke and seasonal variations, and demonstrated that the incidence of stroke increases in winter and spring.23456 Other studies have found no associations between weather and the incidence of stroke.78 However, all of the studies have described differences in temperature between the dates with and without stroke. There have been few reports on stroke incidence according to daily meteorological characteristics, or on the relationship between daily temperature and stroke subtypes. One report described that the incidence of ischemic stroke was significantly higher during summer and early autumn, whereas hemorrhagic stroke was more common in spring and winter in Korea.9 However, the influence of daily temperature on the incidence of stroke or on stroke subtypes has not been reported previously.
This study aimed to determine whether daily temperatures increase the short-term number of stroke patients and stroke subtypes in Seoul, Korea. Data on the daily meteorological conditions around our hospital over a 10-year period were collected, and the number of strokes was compared in different temperature groups.
METHODS
Meteorological characteristics
Meteorological parameters were obtained from the Korean Meteorological Administration. The variables included the maximum and minimum daily temperatures, mean daily temperature, daily temperature range, day-to-day temperature differential, and average humidity for all days between January 1, 2005 and December 31, 2014 in Seoul (n=3,652 days). Seoul experiences four distinct weather patterns during the seasons of spring, summer, autumn, and winter.
The categories of daily temperature were divided by 10-degree Celcius (℃) from the mean temperature. The daily temperatures in Seoul did not conform to a normal distribution, this ensured that the number of days in the highest temperature group were similar to those in the corresponding lower temperature group, which was divided by 5℃.
Identification of cases
In total, 3,480 consecutive patients with acute (<7 days) ischemic or hemorrhagic stroke were admitted to Soonchunhyang University Hospital during the study period. This center is a tertiary hospital centrally located in Seoul. We determined the area within which the emergency medical service system (119) transports patients to our center. The district includes 21 neighborhoods in Yongsan-gu, Jung-gu, west Seongdong-gu, north Seocho-gu, and north Gangnam-gu. The nearest tertiary hospital is located 4.6 kilometers east of our hospital. Therefore, to minimize selection bias, we excluded patients whose residential addresses were outside a 2-kilometer radius of this hospital. The population included 562,513 adult inhabitants (aged >19 years) based on the Korean population census in 2015. Cases of medical emergencies in selected areas are obliged to be transferred to our center according to the 119 guidelines, and can normally reach our center within 10 minutes by car. About 350 patients with acute ischemic stroke are admitted to our center each year, and the area distribution of patients is similar across years. Patients who experienced a stroke outside the study area (n=661), were referred from other districts (n=82), or with missing address information (n=47) were excluded from this study. Transient ischemic attack was excluded from this study due to the uncertainty of diagnosis for the stroke or its subtype (n=116).
The onset time of stroke was accurately prospectively recorded in all cases, and the median time between the last normal time and first abnormal time was regarded as the stroke onset in unclear cases. Cases for which the time between the last normal time and first abnormal time was >24 hours were excluded from the analysis (n=261). Finally, 2,313 cases were analyzed. The mean daily number of strokes was calculated during the study period of 3,652 days. The study design was approved by the Soonchunhyang University Hospital institutional review board before the investigations commenced (IRB No. 2016-04-019).
Stroke subtypes and workups
Stroke subtypes were assessed by a magnetic resonance imaging (MRI)-based algorithm10 with extensive workups including MRI/angiography, echocardiography, and Holter monitoring in all patients. Ischemic stroke subtypes were determined by the TOAST classification as follows: large-artery atherosclerosis (LAA), small-vessel occlusion (SVO), cardioembolic stroke (CE), stroke of undetermined etiology (SUE), and stroke of other determined etiology (SOE).11 Hemorrhagic stroke were classified into intracranial hemorrhage (ICH) and subarachnoid hemorrhage (SAH). Posttraumatic or nontraumatic subdural or epidural hemorrhages were not enrolled in this stroke registry.
Statistical analysis
Descriptive statistical methods were used to characterize the meteorological parameters. One-way analyses of variance (ANOVA) were applied to compare the number of cases among the temperature groups. The mean number of cases for each stroke subtype according to the maximum and minimum daily temperatures was analyzed by ANOVA and Duncan's post-hoc test. The cutoff for statistical significance was defined as p<0.05. All statistical analyses were performed using SPSS (version 18.0 for Windows, SPSS Inc., Chicago, IL, USA).
RESULTS
In total, 2,313 acute stroke cases whose residential addresses were within a 2-kilometer radius of the hospital were identified during the period: 1,643 ischemic strokes and 670 hemorrhagic strokes. The 1,643 ischemic stroke subjects comprised 675 with LAA (41.1%), 248 with SVO (15.1%), 213 with CE (13.0%), 342 with SUE (20.8%), and 49 with SOE (3.0%). The 670 hemorrhagic stroke subjects comprised 326 with ICH (48.7%) and 344 with SAH (51.3%). The meteorological parameters in Seoul between January 2005 and December 2014 are outlined in Table 1. The maximum and minimum daily temperatures were 17.1±10.8℃ (mean±SD) and 9.0±10.7℃, respectively. The mean number of total strokes daily was 0.63.
The mean numbers of stroke cases in each maximum daily temperature group are presented in Table 2. The mean number of stroke cases daily was 0.77 for >32.0℃ (n=124 days), 0.61 for 27.1℃ to 32.0℃ (n=720 days), 0.61 for 17.1℃ to 27.0℃ (n=1,138 days), 0.64 for 7.1℃ to 17.0℃ (n=829 days), 0.63 for -2.9℃ to 7.0℃ (n=731 days), and 0.82 for ≤-3.0℃ (n=110 days). The mean number of total strokes was maximal in the highest and lowest groups of maximum daily temperature (p=0.048). The mean number of ischemic strokes was maximal for the highest maximum daily temperature (p=0.040). The mean number of hemorrhagic strokes did not differ significantly among the maximum daily temperature groups (p=0.082).
The mean numbers of stroke cases in each minimum daily temperature group are presented in Table 3. The mean number of stroke cases daily was 0.75 for >25.0℃ (n=89 days), 0.64 for 19.1℃ to 25.0℃ (n=771 days), 0.60 for 9.1℃ to 19.0℃ (n=1,044 days), 0.64 for -0.9℃ to 9.0℃ (n=927), 0.62 for -10.9℃ to 1.0℃ (n=748 days), and 0.92 for ≤-11.0℃ (n=74 days). The mean numbers of total strokes and hemorrhagic strokes were maximal in the lowest minimum daily temperature group (p=0.020 and 0.020 in each). The mean number of ischemic strokes did not differ significantly among the minimum daily temperature groups (p=0.127).
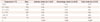
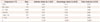
For maximum and minimum daily temperatures, the mean numbers of stroke subtypes are presented in Table 4 and 5. The highest maximum daily temperature was associated with a significantly increased number of LAA cases (p=0.045), and the lowest maximum daily temperature was associated with significantly increased numbers of cases of SVO (p=0.013) and ICH (p=0.029). The distributions of the other subtypes were not significantly affected by the maximum daily temperature. The highest minimum daily temperature was also associated with a higher number of LAA cases (p=0.006), and the lowest minimum daily temperature was associated with a higher number of ICH cases (p=0.019). The other stroke subtypes showed no differences in the mean numbers of cases according to the minimum daily temperature.
The number of stroke cases did not differ significantly with the mean daily temperature, daily temperature range, day-to-day temperature differential, or daily average humidity (data not shown).
DISCUSSION
The possibility of a relationship between meteorological conditions and incidence of stroke has not yet been clarified. Despite the lack of strong evidence that weather conditions influence stroke incidence, many clinicians feel that meteorological conditions do impact the onset of stroke. Although there are some reports of no significant relationships between stroke and daily meteorological conditions,3712 other previous studies have found that cold temperature is associated with an increased risk of stroke occurrence.13141516
The present study found that the number of total stroke patients was significantly associated with the maximum daily temperature being less than -3℃ and with the minimum daily temperature being less than -11℃ in Seoul, Korea. The lowest daily temperature was associated with increased ischemic strokes and hemorrhagic strokes, especially SVO and ICH.
Several mechanisms could be responsible for the risk of stroke incidence being increased for the lowest daily temperature. The blood pressure and the levels of serum cholesterol, C-reactive protein, plasma fibrinogen, factor VII clotting activity in plasma, red blood cells, and platelet counts are reportedly higher at low temperatures.171819 The morning increase in the blood pressure is closely associated with the meteorological conditions.13 The increases in systolic blood pressure are also greater at lower temperatures.20 Considering the association of blood pressure and inflammatory markers with SVO2122 and ICH,2324 cold temperature could influence the occurrence of occlusion or rupture of cerebral small vessels.
On the other hand, the highest daily temperature was mainly associated with an increased number of ischemic stroke patients. A previous study suggested that exposure to heat is likely to cause dehydration, increasing the viscosity of the blood.25 Some experiments involving animal models have suggested that the blood supply to the central nervous system decreases during heat exposure.2627 These effects might not result in abnormalities in subjects without vascular disease, but they could increase the likelihood of thromboembolic episodes in patients with vascular disease. These hypotheses are consistent with our study finding that a larger number of cases of LAA was associated with the highest temperature group.
This study had several limitations and strengths. First, selection or information biases could have been present due to the clinical data being obtained retrospectively from a prospective acute stroke registry. Second, this study involved a single center, although this limitation was offset by the study period being longer and the inclusion of more subjects than in previous studies. Our results need external validation to confirm the association between meteorological parameters and incidence of stroke. However, because the same author managed all data of the stroke cases and meteorological parameters, the data obtained in this study should be accurate and consistent. Third, this study only counted the mean numbers of stroke patients, and did not consider vascular risk factors as covariates that could affect stroke incidence. Finally, the study covered a small geographical area, only including patients who resided within a 2-kilometer radius of our hospital. Seoul is one of the largest cities worldwide with one of the highest population densities. Therefore, covering a larger region might result in heterogeneity of the weather and environment characteristics for the sampled population. In addition, because there are many hospitals in Seoul, patients with acute stroke could visit other nearby hospitals. We therefore thought that conducting a single-center-based study covering a restricted region with similar meteorological conditions could be more suitable than a multicenter study for elucidating the effect of temperature on the occurrence of stroke.
In conclusion, the lowest and highest daily temperatures were associated with increased numbers of stroke patients in Seoul, Korea. The lowest temperature was associated with increases in both ischemic and hemorrhagic strokes, especially SVO and ICH, while the highest temperature was associated with increases in ischemic stroke, mainly LAA. Further studies are warranted to further elucidate the associations and pathophysiological mechanisms underlying the relationships between meteorological characteristics and the occurrence of stroke subtypes.



 XML Download
XML Download