

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Parkinson's disease (PD) is a multisystem disorder that is characterized by a combination of various motor symptoms and nonmotor symptoms (NMS). The motor symptoms associated with PD are well known and are commonly treated by clinicians.123 In contrast, recent studies of NMS have yielded mixed results despite these symptoms increasingly being recognized as an important part of PD symptoms and a significant cause of disability and, consequently, poor quality of life in PD patients.4567 The various NMS in PD can be classified into four domains: neuropsychiatric, sensory, autonomic, and sleep symptoms.8 Among these, rapid-eye-movement sleep behavior disorder (RBD), constipation, depression, and olfactory dysfunction appear during the premotor stages of PD and are often referred to as prodromal signs.4791011 However, other NMS such as cognitive impairment, genitourinary dysfunction, gastrointestinal (GI) dysfunction, sleep disturbance, and visual hallucinations are associated with advancing age and disease severity.7 Accordingly, patients with advanced PD tend to have more severe NMS.6 The health-related quality of life (HrQoL) is considered critical in patients with neurodegenerative disorders, and recent PD research has increasingly focused on factors that affect HrQoL. HrQoL is closely associated with the severity of NMS,121314 and NMS of PD are known to have a greater impact on HrQoL than do motor symptoms.6 Therefore, it is important to determine the NMS status of PD patients in large populations in order to better understand the impact of PD.
In this Nonmotor symptoms And qualiTy of life In ParkinsON's disease (NATION) study, we investigated NMS characteristics and their impact on HrQoL using a nationwide multicenter design. We aimed to determine the prevalence and severity of NMS according to the disease stage, status, and motor subtypes, and also the factors that influence each NMS domain and affect HrQoL.
METHODS
Study design
The NATION study was a cross-sectional investigation that included data from 37 movement-disorders clinics widely distributed throughout South Korea. Principal investigators of participating clinics who were members of the Korean Movement Disorders Society (KMDS) were invited to take part in the study. Each clinic was confirmed to have the ability to implement the study protocol based on its previous participation in clinical studies. The study protocol was approved by the institutional review board of each institute, and all subjects were required to provide informed consent in compliance with the regulations of that board.
Subjects
The study included PD patients and healthy controls who were recruited between March 2012 and January 2013. PD was diagnosed based on the UK Parkinson's Disease Society Brain Bank criteria, and patients were consecutively enrolled according to disease status as follows: 1) de novo group, any stage of PD with no prior anti-PD medications, 2) mild-to-moderate group [modified Hoehn & Yahr (H&Y) stage of ≤3] taking anti-PD medication, and 3) severe group (modified H&Y stage 4 or 5) taking anti-PD medication. To increase the reliability of PD diagnosis, all PD patients were reassessed 6 months after the initial enrollment date. Normal controls were recruited from volunteer caregivers of the patients at the inpatient and outpatient clinics who had no evidence of neurological or serious medical illnesses in their medical history or a neurological examination. The following exclusion criteria were applied: 1) history of systemic disease that might affect NMS or HrQoL (e.g., cancer or organ failure); 2) history of medication that might affect parkinsonism, NMS, or HrQoL; and 3) psychiatric illness or dementia [Mini Mental State Examination (MMSE) score of <20 points] restricting the understanding of the questionnaire.
Methods
We assessed the following demographic characteristics of the patients: sex, age, age at onset, duration of disease, marital state, occupation, and economic status. The modified H&Y stage and the Unified Parkinson's Disease Rating Scale (UPDRS) were used to evaluate the overall severity of disease, including motor disabilities.1516 The clinical motor phenotype was classified according to Jancovic et al.17 The presence of motor complications (motor fluctuation and dyskinesia) was also assessed based on interviews and medical records. NMS were assessed based on the Korean version of the Nonmotor Symptoms Scale (K-NMSS),18 Parkinson's Disease Sleep Scale (PDSS), Beck Depression Scale (BDI), Beck Anxiety Inventory (BAI), and Parkinson Fatigue Scale (PFS). The Korean version of the MMSE (K-MMSE),19 the Korea version of the Montreal Cognitive Assessment (MoCA-K),20 and the Korean version of the Frontal Lobe Assessment Battery (K-FAB)21 were used to evaluate cognitive function. The Korean version of the Neuropsychiatric Inventory Questionnaire (K-NPI)22 was used to assessed behavioral and psychological symptoms. HrQoL was assessed using the Parkinson's Disease Questionnaire-39 (PDQ-39).23 The motor phenotype was determined according to the UPDRS motor score. Each domain of the K-NMSS was used to assess the severity of NMS.
Statistical analysis
The SPSS software package (version 15.0K for Windows, SPSS Inc., Chicago, IL, USA) was applied for all statistical evaluations. ANOVA was used for comparisons of groups conforming to normal distributions, while the Mann-Whitney U and Kruskal-Wallis tests were used to compare variables that did not conform to a normal distribution. All comparisons between groups for each variable were carried out using Fisher's exact test, and linear-by-linear associations were determined with Bonferroni's post-hoc analysis. Spearman's rank correlation coefficients were used to identify associations with other variables. Logistic regression analysis was used to assess the relative contributions of clinical variables to the total K-NMSS score. A difference was considered significant when the p value was <0.05.
RESULTS
Demographic and clinical background information
In total, 323 PD patients [153 men, 170 women; age, 66.80±9.64 (mean±SD) years; median age, 69 years] and 94 healthy controls (33 men, 61 women; age, 62.96±9.39 years; median age, 64 years) were enrolled in the study. The demographic and clinical characteristics of the participants are presented in Supplementary Table 1 (in the online-only Data Supplement). The most common occupation was farming (n=286, 64.4%). The PD patients were divided into three subgroups: de novo PD (n=121), early PD (n=142), and advanced PD (n=60), in which the H&Y stages were 1.88±0.75, 2.05±0.61, and 4.12±0.32, respectively. The PD patients were classified according to motor phenotype into the 1) tremor-dominant (TD) group (n=27), 2) intermediate group (n=32), and 3) postural instability and gait disturbance (PIGD) group (n=264). As indicated in Supplementary Table 1 (in the online-only Data Supplement), there were significant differences between PD patients and healthy control in scores on the PDSS, BDI, BAI, PFS, K-MMSE, MoCA-K, K-FAB, and K-NPI. The PDSS scores did not differ significantly between the PD subgroups. The BDI scores indicated that the depression severity was significantly greater in the advanced PD group than in the de novo PD and early PD groups. Analysis of the BAI scores indicated that anxiety was more severe in the advanced PD group than in the de novo PD group; however, the BAI score did not differ significantly between the de novo PD and early PD groups or between the early PD and advanced PD groups. The PFS score was higher in the advanced PD group than in the de novo PD group, but did not differ significantly between the de novo PD and early PD groups or between the early PD and advanced PD groups. Analysis of the K-MMSE scores indicated that global cognitive dysfunction occurred more frequently in the advanced PD group than in the de novo PD and early PD groups, but that its prevalence did not differ significantly between the de novo PD and early PD groups. However, comparison of the MoCA-K and K-FAB scores showed significant differences only between the early PD and advanced PD groups. These results are summarized in Supplementary Table 2 (in the online-only Data Supplement).
NMS scale scores in the PD and control groups
The prevalence of NMS and mean scores on the K-NMSS in the PD and normal control groups are presented in Table 1. The prevalence of NMS was significantly higher in PD patients (98.1%) than in the control group (73.4%) for all K-NMSS domains. All of the K-NMSS domain scores were significantly higher in PD patients than in the normal controls. The mean number of NMS in PD patients was 5.27 out of 12 domains. The mean number of affected K-NMSS domains was higher in advanced PD patients (6.73) than in de novo PD patients (4.38) and early PD patients (5.40). The most common K-NMSS domains affecting PD patients were the sleep/fatigue (82%), mood/cognition problems (79.3%), attention/memory problems (77.4%), and urinary dysfunction (73.7%), with perception problems/hallucination (23.8%), weight change (25.4%), and excessive sweating (29.7%) being less frequent. In addition, compared with the control group, the PD patients showed higher prevalence ratios for perception problems/hallucination, weight change, pain, GI dysfunction, and taste/smell function, with PD-to-control ratios of 7.44, 5.91, 3.77, 3.15, and 3.04, respectively. The total score on the K-NMSS was higher (51.1±53.0) in the group with a higher PD onset age (>65 years, n=211) than in the group with an age at onset of <5 years (36.6±35.8). The former group also had higher scores in the dysautonomic domain, including (in descending order) cardiovascular, GI, and urinary dysfunctions, sleep/fatigue, and perception problems/hallucination.
NMS scale based on PD stage
The total number of affected K-NMSS domains increased with the PD stage. There were considerable differences in the total number of affected domains even in the de novo PD and control groups. Each K-NMSS domain score was significantly higher in the advanced PD group than in the de novo PD and early PD groups, with the exception of pain (Table 2, Fig. 1).
NMS prevalence according to motor subtype
The prevalence of NMS and NMS domain scores according to motor subtype are presented in Table 3. Only the GI symptoms were more frequent in the PIGD than the TD subtype. Additionally, the GI score was the only symptom that was significantly worse in the PIGD than the TD subtype. Although the scores in the other NMS domains tended to be worse in the PIGD subtype than in the TD subtype, the results were not statistically significant. The number of affected NMS domains did not differ significantly with the motor PD subtype.
NMS scale domain and association with clinical variables
After adjusting for age, all K-NMSS domains were significantly correlated with disease duration and all NMS, with the exception of the mood/cognition domain, which was correlated with the total PD motor score (UPDRS part III score) and the total levodopa equivalent dosage (LED). However, after adjusting for disease duration, the total LED was not correlated with any of the K-NMSS domains (Supplementary Fig. 1 and Table 3 in the online-only Data Supplement). Table 4 presents the association between K-NMSS and each clinical variable based on multiple regression analysis. The disease duration and a depressive mood on BDI significantly affected all of the K-NMSS domains. Specific variables were significantly correlated in each domain: LED with sleep/fatigue and sexual dysfunction; cognitive status on K-MMSE with cardiovascular symptoms; PDSS with attention/memory problems, perception problems/hallucination, and urinary dysfunction; anxiety on BAI with attention/memory problems and excessive sweating; and fatigue on PFS with attention/memory problems, weight change, and taste and olfactory dysfunctions.
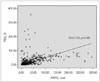
NMS scale and HrQoL
The total K-NMSS scores were significantly correlated with HrQoL as assessed using a PD-specific questionnaire (PDQ-39) (Fig. 2) (Supplementary Table 4 in the online-only Data Supplement). The sleep/fatigue and mood/cognition domains in K-NMSS were the most important factors affecting the HrQoL in PD subjects (rS=0.528 and rS=0.573, respectively). In the PD subgroup analysis, sleep/fatigue and mood/cognition were the primary factors in the de novo and early PD groups. Attention/memory and mood/cognition were the most important factors for HrQoL in the advanced PD group, while miscellaneous variables and the sleep/fatigue domain were less likely to be correlated with HrQoL status. Finally, the perception problems/hallucination domain negatively impacted HrQoL in advanced PD but not in de novo or early PD.
DISCUSSION
Our analysis of various aspects of the clinical presentation of NMS in PD has demonstrated that PD subjects show significant differences in the scores on mood, cognition, and sleep questionnaires compared with healthy controls. These findings suggest that PD is not simply a movement disorder, but instead is a systemic disorder that includes both motor symptoms and NMS, which would be due to the degeneration of nigrostriatal-extranigral systems.2425 Although the importance of NMS in PD has been recognized recently, these symptoms have remained underreported by patients and overlooked by clinicians.526 Because NMS greatly impact the quality of life and can be a great burden for patients and their families,6827 it is important to assess the complexity of NMS. The NMS of PD are heterogeneous and present with a variety of manifestations that can be classified in several ways, such as according to disease stage based on pathological progression,28 according to symptomatic similarities, or according to major causative neurotransmitters.293031 We identified tendencies of the NMS in the present study regardless of the specific underlying mechanism. The PD group showed both a higher prevalence and a higher score in all K-NMSS domains compared with the controls. Sleep/fatigue, mood/cognition, attention/memory, and urinary dysfunctions were the most commonly reported NMS in PD patients. However, these domains were not specific to the study groups, being also prevalent in the control group, which indicates that the prevalence rates of NMS need to be interpreted cautiously in clinical practice. Our analysis of a prevalence ratio revealed that the PD group exhibited a higher ratio for perception problems/hallucination, miscellaneous symptoms (weight change, taste/smell, and pain), and GI dysfunction compared with the other domains, indicating that these domains are more specific to PD. Accordingly, there were several prevalent NMS that were correlated with the participants' age, such as urinary and sleep symptoms, which were not specific to the PD patients.
In our study, 98.1% of the PD patients showed at least one nonmotor symptom, and most commonly presented with sleep/fatigue issues, which is similar to the results of an Italian study.12 While urinary dysfunction was the fourth most common of the NMS in our study, several previous studies have found urinary dysfunction (nocturia or urgency) to be the most common NMS domain.5632 In our survey, the prevalence of urinary dysfunction (73.7%) was not lower than in previous studies (54.5–68.4%),83233 but the affective symptom scores in the baseline characteristics were high, although not compatible with a diagnosis of mood disorders, which can explain why sleep/fatigue and mood/cognition symptoms were more common than urinary dysfunction. This is similar to a previous study finding that more of the K-NMSS domains were affected as the disease progressed.12 It is also compatible with research findings that NMS are intrinsic to PD but are also correlated with the involved structures and related to drugs taken as the disease progresses.72434 We identified significant differences in the number and prevalence of involved NMS even in the de novo and early stages of PD compared with controls. Meanwhile, there were no statistically significant differences in K-NMSS domains in early PD stages and similar stages in the de novo PD group, which indicated that NMS in PD largely appear in later stages rather than being evenly distributed throughout the disease course.35 Previous investigations have found obvious differences in clinical manifestations, prognosis, and drug responsiveness according to the PD motor phenotype.3637 Although the pathophysiological basis is still unknown, disparity in the patterns of dopaminergic cell loss, differences in other neurotransmitter systems, deposition of amyloid plaque, and brain atrophy have been proposed as explanations for differences in PD subtypes.38394041 In the present study, the affected K-NMSS domains did not differ significantly according to the PD phenotype between groups, with the exception of GI dysfunction. This contrasts with Khoo et al.42 reporting that even in early PD, a larger number of NMS were involved in the PIGD group. Another recent study found no significant difference in a larger PIGD and TD group comparison.43 In our study, there was a tendency—although not statistically significant—for the prevalence and number of affected NMS domains to both be higher in the PIGD subtype. However, there was a significant difference in the numbers of PD phenotypes, in that 82.3% of the recruited patients were of the PIGD subtype.
When the results were adjusted for age, nearly all of the K-NMSS domains were correlated with disease duration, total LED, and motor status as assessed by UPDRS part III scores. However, after adjusting for the disease duration, the total LED was not correlated with any NMS. These results indicate that disease duration is more important than the LED to NMS in PD. The presentation of NMS varies, and patients present at various stages. Several NMS such as olfaction problems, RBD, constipation, and depression have been suggested to be preclinical features of neurodegenerative diseases.81011 In addition to these intrinsic features, additional NMS can develop as the disease progresses, and these can significantly affect the patient's condition.372444 It is therefore possible that the disease duration contributes to the prevalence and severity of NMS.454647 The NMS of PD can also be influenced by accompanying problems. Some NMS of PD are known to result from dopaminergic deficits, while other NMS do not respond to dopaminergic treatment.48 Duration and depressive mood consistently affected all K-NMSS domains, and each K-NMSS domain was influenced by specific clinical variables in the present study, as indicated in Table 4.
Clinicians are primarily focused on motor symptoms, which may result in them overlooking NMS or HrQoL.49 However, NMS are a major determining factor of HrQoL in PD.133250 Gallagher et al.6 insisted that NMS can have a greater effect than motor features on some aspects of HrQoL in PD. Mood/cognition and sleep/fatigue were the main factors associated with HrQoL in all of the PD subjects in the present survey. These results are similar to other studies finding that depression is a major detrimental factor for HrQoL in PD.1451 The subgroup analysis indicated that the mood/cognition domain is a common factor that can determine HrQoL for the overall PD group, but that sleep/fatigue contribute to de novo and early PD only, while the perception problems/hallucination and attention/memory domains are specific for advanced PD. These observations suggest that the presentation of NMS differs according to disease stage, and that NMS attributed to HrQoL status are also influenced by disease stage. This result is comparable to a previous report of HrQoL associated with NMS varying according to the disease duration, and mood, sleep, fatigue, and autonomic symptoms negatively affecting NMS with regard to HrQoL in PD.6
The burden experienced by PD patients is correlated with the number of NMS.27 Some NMS, such as depression, constipation, and urinary and sleep dysfunctions, can be improved by the active treatment of parkinsonian features.8 Accordingly, HrQoL can also improve during NMS treatment.42652 For these reasons, increasing the recognition of nonmotor aspects of PD is warranted for improving the HrQoL of affected subjects, and tailored treatment strategies for diverse stages of PD should consider NMS.
There were some limitations to this study. First, we did not analyze the presence of motor complications in the advanced PD group. Since motor complications in PD are significantly associated with NMS,53 it is important to assess the effects of drug-related motor complications. However, we analyzed the correlations between the LED and K-NMSS domains in order to elucidate the effects of this drug on NMS in PD. Second, most of the enrolled PD subjects were the PIGD type, which does not adequately represent the whole PD population; however, the PD phenotype analysis formed only a small part of our study, and the results are applicable to a large PD population.
This was a multicenter, nationwide, representative study of Korean patients with a case-control comparison design. The diagnostic accuracy of the study was increased by reconfirming the clinical diagnoses at 6 months after the initial diagnoses. Another strong point is that our nationwide Korean survey is one of the first large cross-sectional studies to elucidate the overall features and influences of nonmotor aspects of PD. The results from this study have highlighted the impact of NMS, which could allow the earlier detection of this degenerative disease, and thereby facilitate better therapeutic plans and improve the HrQoL of PD patients.





 XML Download
XML Download