

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
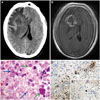
A 50-year-old man presented to the emergency room with a 10-day-long clinical picture of behavioral disturbances and pharmacorefractory headache. His past medical history was remarkable due to a 8-month course of constitutional syndrome with normal results in a blood test, thoraco-abdomino-pelvic computed tomography (CT) scan, and colonoscopy. A neurological examination only highlighted drowsiness, but cranial CT (Fig. 1A) and subsequent magnetic resonance imaging (MRI) (Fig. 1B) showed a right-side frontoparietal infiltrative mass with annular enhancement invading the contralateral hemisphere through the corpus callosum, causing a midline shift. After performing a stereotactic lesion biopsy, immunohistopathology revealed Toxoplasma intracellular bradyzoites and extracellular tachyzoites (Fig. 1C and 1D). Moreover, immunocytochemistry using an anti-human immunodeficiency virus (HIV) p24 antibody demonstrated the presence of HIV antigen (Fig. 1E). Laboratory analyses disclosed positivity for antitoxoplasma immunoglobulin G, with CD4 at 262 cells/µL and a viral load of 747.604 copies/mL. Antitoxoplasma and antiretroviral therapies were initiated, and the patient eventually achieved partial remission.
Glioblastoma is the most common type of primary brain neoplasm in adults,12 while toxoplasmosis is produced by the coccidian Toxoplasma gondii (T. gondii). The final parasite hosts are cats and other feline species. Human toxoplasmosis infection is usually contracted from the consumption of undercooked meat or contact with cat feces containing parasitic cysts. The prevalence of T. gondii seropositivity differs widely, ranging from 20–40% in United States to 70% in Haiti and Brazil. In addition, T. gondii is an obligate intracellular protozoan parasite with a tendency to infect the central nervous system (CNS). The vast majority of primary infections in immunocompetent individuals are asymptomatic. Some people develop lymphadenopathies, but although T. gondii may encyst and remain dormant in the CNS, symptomatic neurological disease is rare.3 Furthermore, toxoplasma encephalitis (TE), which is an acquired immune deficiency syndrome (AIDS)-defining illness, is generally a late complication of HIV infection that usually results from latent infection reactivation, and its onset rarely precedes a diagnosis of HIV infection. Common TE clinical presentations of CNS symptomatic disease are variable, and may include cephalalgia, sleepiness, disorientation, nonspecific features of raised intracranial pressure, and progressive focal neurological deficits, with or without fever. Only 21.4% of patients reportedly show a single lesion, and AIDS patients may have TE in abnormal locations.24 A definitive diagnosis requires a brain biopsy, with this highly invasive procedure being absolutely justified in situations of atypical clinicoradiological context for TE, and in cases of neurological deterioration despite the administration of antitoxoplasma therapy.5 In this regard, diffusion MRI sequences may be useful, and cerebral abscess should be suspected in all cases of cystic or necrotic masses with hyperintensity signals in diffusion sequences and a low apparent diffusion coefficient.6 The Toxoplasma loose tachyzoites and encapsulated bradyzoites around necrotic lesions usually ap pear abundant under an optical microscope, as shown by the blue and green arrows, respectively, in Fig. 1C for staining with hematoxylin and eosin (HE). They are oval- or crescent-shaped and may appear clustered together within cells (in vacuoles or pseudocysts) or lie free inside the cell cytoplasm. Toxoplasma zoites formations are reasonably easy to identify when stained with HE; however, but when they are identified and distinguished immunohistochemically (dark-brown stain for antitoxoplasma antibody in Fig. 1D), a definitive diagnosis of toxoplasmosis is possible.34
Based on the current literature, this is the first described case with these neuroradiological features and a CD4 level of >200 cells/µL heralding AIDS. Hence, clinicians must consider this possibility before a ring-enhancing space-occupying cerebral lesion, even in patients without prior immunosuppression or an HIV infection history, in order to accomplish early diagnosis and proper treatment administration.
 XML Download
XML Download