

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Parkinson's disease (PD) and multiple-system atrophy of the parkinsonian type (MSA-P) are two progressive neurodegenerative disorders that in addition to similar motor symptoms also present with symptoms of dysautonomia. Among the various symptoms of autonomic dysfunction, orthostatic hypotension (OH) is a common presentation in both of these disorders.123 It has been suggested that despite their autonomic symptoms being similar, the underlying pathophysiological mechanisms are different.45 Several studies have examined the baroreflex sensitivity (BRS) as a measure of autonomic function in PD and multiple-system atrophy (MSA). Some studies have shown BRS to be similarly low in PD and MSA.567 while others have shown it to be significantly smaller in MSA.8
These previous studies are subject to a few important caveats. Some of them assessed the BRS using a spontaneous method while others used a reflexive method, with no comparison being performed between the two. It is well documented that MSA-C patients (MSA of the cerebellar type) and MSA-P patients show differences in both the severity and onset of OH9 and it is noteworthy that several studies combined these patients in their analyses.78 It has also been demonstrated that BRS is lower in Parkinson's disease patients with orthostatic hypotension (PDOH) than in those without OH510 and that a lower BRS is correlated with a higher score on the Hoehn and Yahr scale of severity.8 BRS has also been shown to differ between males and females.1112 However, the groups included in all of the previous studies were heterogeneous in nature and the confounding factors were not taken into consideration.
In the present study we assessed the BRS as a spontaneous response (spontaneous BRS) and as a cardiovagal reflexive response (cardiovagal BRS) using the Valsalva maneuver (VM) in male PDOH patients with a score on the Hoehn and Yahr scale of 1–3 and in male patients with multiple-system atrophy of the parkinsonian type (MSA-POH) both the groups having OH, taking care to maintain homogeneity in the groups. We also examined the sympathetic and parasympathetic modulation of the heart and the vasculature by measuring the heart rate variability (HRV) and the blood pressure variability (BPV).
METHODS
Patients with PD diagnosed using the United Kingdom Brain Bank criteria13 and with MSA-P diagnosed using the Second Consensus Criteria 200814 were recruited from the Neurology Outpatient Department of the All India Institute of Medical Sciences (AIIMS), New Delhi, India. Patients with cerebrovascular and/or cardiovascular diseases and PD patients with scores on the Hoehn and Yahr scale of 4 or 5 were excluded from the study. The recruited patients were queried in interviews for the presence of symptoms of OH, which resulted in 16 PD patients and 22 MSA-P patients being selected and then tested for the confirmation of OH using a head-up tilt test in the Autonomic and Vascular Function Laboratory of the Department of Physiology, AIIMS (Table 1).
The study was conducted from April 2012 to November. Subjects were included in the study only after they had provided written consents. All subjects were asked to refrain from exercise and from consuming alcohol, caffeine, and nicotine for at least 4 hours prior to the tests.
Protocol
Three-lead electrocardiography (ECG) was used to measure the heart rate and the interbeat interval. The beat-to-beat blood pressure was measured by finger photoplethysmography (Finometer ® model 2, Finapress Medical Systems, Amsterdam, the Netherlands). After 15 min of rest, ECG lead II and beat-to-beat blood pressure recordings were made for 5 min in the supine posture. The data were used to assess BRS as well as for power spectral analysis. After a 2-min rest in the sitting position, the subjects were asked to perform the VM at an expiratory pressure of 40 mm Hg for 15 s. Simultaneous ECG and beat-to-beat blood pressure recordings were then made.
Spontaneous BRS
The spontaneous BRS was computed from continuous interbeat interval recordings of the ECG and beat-to-beat changes in blood pressure using Nevrokard software. The BRS was quantified using the sequence method that is based on computer-based identification of spontaneously occurring sequences of three or more consecutive beats characterized by either a progressive rise in blood pressure and lengthening of the R-R interval or by a progressive decrease in blood pressure and shortening of the R-R interval. The criteria used for identifying the sequences were an R-R interval variation of greater than 5 ms, BP changes greater than 0.5 mm Hg, sequences longer than three beats, and a sequence correlation coefficient greater than 0.85.15
Cardiovagal BRS
Analyses were performed during phases II and IV of the VM. Systolic blood pressure values were linearly regressed against the corresponding R-R intervals on a beat-to-beat basis. The cardiovagal BRS was quantified from the slope of the relationship between the cardiac interbeat interval and the systolic blood pressure during phase II of the VM.7 In phase IV, the cardiovagal BRS was quantified from the point at which the R-R interval began to lengthen and continued to the point of maximum elevation of the systolic blood pressure. The slope of the relationship between the R-R interval and the systolic blood pressure was used as a measure of cardiovagal BRS if the correlation coefficient exceeded 0.80.16
Spectral analysis of heart rate variability and blood pressure variability
Short-term HRV was quantified from 5-min ECG recordings using a recommended method17 implemented in Nevrokard HRV software (version 6.2.0, Slovenia). Briefly, consecutive R-R intervals were obtained from ECG recordings followed by quantification of HRV in the time domain and analysis in the spectral (frequency) domain. Time-domain measures included the standard deviation of all normal R-R intervals, the root-mean-square standard deviation, the difference between adjacent R-R intervals of more than 50 ms, and the percentage difference between two consecutive R-R intervals of more than 50 ms. Frequency domain measures were obtained using Fast Fourier Transform technique to quantify power in 2 bands i.e. low frequency (LF) 0.04–0.15 Hz, and high frequency (HF) 0.15–0.40 Hz followed by calculation of LF/HF ratio. Total power was estimated with the sum of the frequencies.17
Short-term BPV was computed in the time and frequency domains using methods in Nevrokard software similar to those used for HRV.
RESULTS
Spontaneous baroreflex sensitivity
The BRS obtained by the spontaneous method was found to be similar in PD and MSA-P patients. The BRS systolic blood pressure was 5.04±0.66 ms/mm Hg in PD and 4.78±0.64 ms/mm Hg in MSA-P (p=0.54) (Fig. 1A); the corresponding values for the BRS mean blood pressure were 7.40±1.14 ms/mm Hg vs. 7.23±0.71 ms/mm Hg (p=0.89).
Cardiovagal baroreflex sensitivity
Data obtained in phases II and IV of the VM were assessed. Only 6 out of 16 PD and 8 out of 22 MSA-P patients were able to perform the maneuver in accordance with the protocol. The baroreflex-cardiovagal gain in phase II of the VM did not differ significantly between PD and MSA-P (0.96±0.75 ms/mm Hg vs. 1.34±1.51 ms/mm Hg, p=0.76) (Fig. 1C). However, the BRS in phase IV was lower in PD patients than in MSA-P patients (0.03±0.07 ms/mm Hg vs. 2.86±2.39 ms/mm Hg, p=0.004) (Fig. 1B).
Power spectral analysis
Heart rate variability
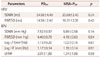
The LF/HF ratio was significantly higher in PDOH patients than in MSA-POH patients (2.36±1.06 vs. 1.77±1.97, p=0.05) (Fig. 2). LF and HF indices of the HRV did not differ between PDOH and MSA-POH (1.78±0.21 ms2 vs. 1.67±0.14 ms2, p=0.66; and 1.45±0.18 ms2 vs. 1.64±0.17 ms2, p=0.47; respectively) (Table 2).
Blood pressure variability
Spectral analysis of the blood pressure showed that the LF power was significantly higher in PDOH patients than in MSA-POH patients (1.65±0.13 mm Hg vs. 1.0±0.12 mm Hg, p=0.0013). The LF power of the R-R interval was similar in the two groups. The HF power of the blood pressure and the R-R interval did not differ significantly between PDOH and MSA-POH (Table 2).
DISCUSSION
The spontaneous BRS did not differ significantly between the PDOH and MSA-POH patients in this study. However, the BRS quantified as the reflexive cardiovagal responsiveness (cardiovagal BRS) in phase IV of the VM was significantly lower in PDOH patients than in MSA-POH patients.
To the best of our knowledge this is the first report of the spontaneous BRS being similarly low in PDOH and MSA-POH. Friedrich et al.8 reported that BRS was lower in MSA than in PD. That study grouped the PD patients together irrespective of the disease severity and the presence or absence of OH, and found an inverse correlation between the spontaneous BRS and disease severity. This is further supported by Barbic et al.10 finding that BRS was lower in PDOH patients than in PD patients without OH. The results of our study differed from those of Friedrich et al.8 because we had excluded confounding factors by recruiting a group of PD patients who were homogeneous with respect to the severity of the disease and the presence of OH. The presence of OH and the similarity of the disease severity in the PD patients could explain why the spontaneous BRS was similar in the PD and MSA-P patients in our study.
Our findings for the cardiovagal BRS in phase II of the VM are consistent with Goldstein et al.5 finding no difference between PDOH and MSA-POH patients. However, we found that the cardiovagal BRS in phase IV of the VM was lower in PDOH than in MSA-POH. One strength of the present study is that the cardiovagal BRS in phase IV of the VM has not been reported previously for either PDOH or MSA-POH patients. During phase IV, the blood pressure increases due to the sudden increase in the venous return, resulting in a decrease in the heart rate induced by activation of the vagal component of autonomic control. This differs from the cardiac response in phase II, which is primarily due to parasympathetic withdrawal in the early phase and activation of the sympathetic component in the late phase.18 Our study showed that the cardiovagal BRS in phase IV is lower in PDOH than in MSA-POH. This could be due to either a compromised sympathetic response in MSA-POH patients or poor parasympathetic activity in PDOH patients. This finding is related to a recent report of α-synuclein deposition in the dorsal motor nucleus of the vagus occurring earlier in PD than in MSA-P.1920 In contrast, sympathetic denervation has been shown to be present in both PD and MSA-P.2122
The HRV showed a significantly higher LF/HF ratio in PDOH patients than in MSA-POH patients. This may reflect either hyperactivity of the sympathetic system or hypoactivity of the parasympathetic system in PDOH patients. However, the LF and HF values did not differ between the two diseases, which makes it difficult to comment on the sympathetic and parasympathetic components of the autonomic tone. The lower component of the systolic blood pressure in MSA-POH patients compared to PDOH patients predicts a comparatively poor sympathetic response in the former. These results are similar to those obtained by Friederich et al.,8 and they probably explain the low LF/HF ratio obtained during HRV in MSA-POH patients.
The similarly low spontaneous BRS indicates a compromised baroreflex activity in resting conditions in both patient groups. The significantly lower cardiovagal BRS and significantly higher LF/HF ratio from HRV are indicative of severe sympathovagal imbalance in the PHOH patients. The LF and HF values did not differ between PDOH and MSA-POH, and hence no difference in the sympathetic or parasympathetic activity of the autonomic nervous system in resting conditions is indicated. However, the reflexive parasympathetic reactivity as obtained from the low cardiovagal BRS in phase IV of the VM in PDOH is found to be compromised relative to MSA-POH. It is possible that the significantly lower cardiovagal BRS in PDOH relative to MSA-POH is due to hyperactivity of the sympathetic system in MSA-POH, but in that case the cardiovagal BRS in phase II also should have been significantly higher in MSA-POH. Hence it can be postulated that the parasympathetic reactivity is compromised more in PDOH than in MSA-POH.
The main limitation of the study was that relatively small proportions of the PD and MSA-P patients were able to perform the VM in accordance with the standard protocol. This is understandable since these patients have poor motor control. However, these findings open up the opportunity for further investigations in larger populations with certain modifications. A previous study used a lower pressure (30 mm Hg) and shorter duration (12 s) for the VM,7 and such modifications may allow more patients to perform the maneuver. However, we could not lower the limits for the increase in pressure during the VM since this could have influenced the results obtained.



 XML Download
XML Download