

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cholinesterase inhibitors are now widely prescribed for the treatment of mild to moderate Alzheimer's disease (AD), and they produce significant cognitive and functional improvements compared with placebo.1 The positive effect of cholinesterase inhibitors on cognition and activities of daily living (ADL) in patients with mild to moderate AD has been well demonstrated in many clinical trials.2,3,4 This benefit is thought to be mediated through improvement in attention via the actions of cholinesterase inhibitors.5,6
Attention is defined as the mental process of focusing on one stimulus while ignoring others. It serves as a basis for other mental operations including memory and executive function. Impaired attention causes disruption of working memory and other cognitive functions. Theoretically, galantamine is likely to be particularly useful for enhancing attention via modulation of nicotinic receptor activity. However, few drug trials of galantamine for AD have investigated its effect on attention.
Measurement of attention is sometimes challenging with conventional pencil-and-paper tests, since the level of performance on attention can be difficult to capture objectively, especially when there is poor cooperation from demented patients. Computerized tests, and particularly the choice reaction time, are considered a good way to circumvent this problem. The choice reaction time reflects simple selective attention. Attentional function declines in the course of AD, and impairments in dual task performance have been well demonstrated by computerized attention tests.7 In AD, divided attention is considered to be one of the most sensitive cognitive operations that are impaired.8 Thus, in addition to simple attention, complex attention-such as divided attention-could serve as a tool for assessing the treatment response to galantamine. Divided attention is difficult to measure using a computerized system, and no suitable software applications are available. This prompted us to develop our own computerized test program, which taps into various aspects of attention from simple reaction time to divided attention.
The purpose of this study was to determine, using computerized tests, whether galantamine improves attention, and to elucidate whether its effect on attention can be correlated with a beneficial effect on cognition and ADL in patients with mild to moderate AD.
Methods
Patient population
Data were derived from a multicenter study starting in late 2006 involving elderly individuals with dementia in South Korea. The study was conducted in five centers in the metropolitan Seoul area. The participants in the present study met the criteria for probable AD established by the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer's Disease and Related Disorders Association.9 The following patient inclusion criteria were applied: 1) aged 50-85 years; 2) a score of 10-24 on a Korean version of the Mini-Mental State Examination (MMSE); 3) mild to moderate dementia (defined as impairments in ADL resulting from impaired cognition), as determined by evaluations such as a complete medical history, physical and neurologic examinations, and neuropsychological batteries; 4) submitted to an MRI scan; 5) underwent a standard laboratory dementia screen (complete blood counts, blood chemistry panels, vitamin B12/folate levels, syphilis serology, and thyroid function tests); 6) provision of written informed consent; and 7) a primary caregiver who was able to supervise the patient throughout the study, and to provide input as to the efficacy assessments in accordance with all protocol requirements.
Patients with degenerative etiologies other than AD, including idiopathic Parkinson's disease, diffuse Lewy body disease, corticobasal degeneration, and progressive supranuclear palsy, were excluded, as were patients 1) with multiple lacunar/territorial infarctions suggestive of vascular dementia; 2) with a history of significant hearing or visual impairment that rendered interview participation difficult; 3) with a history of neurological disorders or psychiatric illnesses; 4) who had taken acetylcholine esterase inhibitors within 30 days of the beginning this clinical trial; or 5) who had taken psychotropic medications or who had a history of significant alcohol and/or other substance abuse.
This study was conducted in accordance with the Declaration of Helsinki and good clinical practices. The study protocol and informed consent form were reviewed and approved by the Institutional Review Board at each center before study commencement. Prior to enrollment in the study, both the patients and their legal representatives provided written informed consent to participate in the study.
Study design
This was a 12-week, open-label, single-arm, multicenter, prospective study. The changes in attention after 4 weeks of galantamine administration and at the end of the study (i.e., 12 weeks) were measured to determine the relative improvements in attention at those two time points. Attention was assessed with computerized tests consisting of simple and choice reaction-time tests. In addition, divided attention was measured by applying the computerized test for choice reaction time while repeating verbatim prerecorded spoken words produced by a computer. The differences in time taken to achieve dual tasks were considered to reflect divided attention.
Simple/choice reaction times were measured at 4 and 12 weeks. Patients who exhibited any significant improvement in attention at 4 weeks were labeled "early responders", and those who exhibited any significant improvement in attention at 12 weeks were labeled "late responders". The causal relationship between improvement in attention and amelioration of cognition and ADL deficits was also assessed by determining whether there was any association between the attention test results at 4 weeks and those of cognition and ADL measures at 12 weeks.
Tolerability and safety assessments
Safety evaluations included monitoring adverse events (AEs) and clinical laboratory findings.
Efficacy measurements
The MMSE was administered at baseline and weeks 4 and 12 after the commencement of galantamine therapy. Other cognitive measures were collected at baseline and at the end of the study, including the score on the Alzheimer's Disease Assessment Scale-cognitive subscale-11 items (ADAS-cog11). In addition to the cognitive evaluations, the overall severity of dementia was measured using the Clinical Dementia Rating (CDR) scale, and ADL were assessed using the Seoul Instrumental Activities of Daily Living (S-IADL) and the Korean version of the Disability Assessment for Dementia (DAD-K) tool at baseline and at the end of the study.
General attention was measured using the computerized test. The simple reaction-time test measured reaction time to respond to the computer screen changing from a black to a white color. Subjects were asked to perform 70 trials over a 6-minute period. The reaction time and frequency of errors were measured. The choice reaction time involved a series of cards, whereby a single card was presented in the center of the screen and then four similar-looking cards were presented-the subject was asked to choose the card that corresponded with the previously presented single card (Fig. 1). For divided attention, patients were asked to perform the same simple and choice reaction-time tests while repeating the words verbatim that were simultaneously being broadcast from the computer speaker. The differences in the test times measured with and without repeating these words were calculated.
Statistical analysis
It was calculated that a sample size of 94 patients would be needed to detect a clinically relevant difference in S-IADL score with a β level of 0.20, an α level of 0.05, a correlation of moderate level with two-tailed analysis of 0.30, and a 10% dropout rate. The data of all subjects who were enrolled in this trial and took the study medication were used for intention-to-treat (ITT) analysis and safety analysis. Among the subjects involved in the ITT analysis, the data of those who did not violate the study protocols and had no missing values in the efficacy measurements were chosen for the per-protocol (PP) analysis.
Descriptive statistics were used to summarize baseline and end-of trial demographic and cognitive measurements. Changes in cognitive and ADL measurements between at baseline and the end of the trial were evaluated using the paired t-test, in the PP analysis group. As a first step, correlation analyses were performed between changes in choice or simple reaction time and changes in various measures including ADAS-cog11, DAD-K, S-IADL, and MMSE scores, using Pearson's correlation. Next, responder analyses were conducted by comparing the distribution of frequencies of good responders in ADAS-cog11, DAD-K, and S-IADL in quartiles of choice or simple reaction times over the first 4 weeks of taking the trial medication. A "good responder" was predefined as an improvement of ≥4 in ADAS-cog11 score,10,11 no worsening of the DAD-K score,10,12 and no worsening of the S-IADL score,13,14 respectively. The significance of responder analyses was measured using Fisher's exact analysis or chi-square analysis as appropriate.
The statistical analyses were performed using IBM SPSS (version 19.0.1, IBM, Armonk, NY, USA). The cutoff for statistical significance was set at p<0.05 (two-tailed).
Results
Study population and disposition
A total of 92 patients participated in this open-label, single-arm trial; the data from all of these patients was subjected to ITT analysis. During the trial period, 19 participants violated the protocol or withdrew from the study, so that the PP analysis was performed using data from the remaining 73 patients who successfully completed the trial. The baseline characteristics of both analysis groups are listed in Table 1; no significant difference was detected between the characteristics of the two groups.
Efficacy
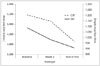
After 12 weeks of taking the trial medication (galantamine) there were significant decreases in both choice reaction time (baseline, 5,216±3,650 sec; 12 weeks, 4,139±2,920 sec; p<0.01) and simple reaction time (baseline, 1,089±782 sec; 12 weeks, 908±606 sec; p<0.01), as displayed in Fig. 2. The reaction times at 4 weeks (5,157±4,848 sec and 982±590 sec, respectively) did not differ significantly from that at baseline (p=0.60 and 0.19, respectively).
The neuropsychological function profiles recorded before and after taking the trial medication are given in Table 2. Neuropsychological function was compared using data from the PP analysis group, for which test scores were available for both the start and end of the trial period. Attention function, measured by choice and simple reaction times, was significantly improved by 12 weeks of the clinical trial. ADAS-cog11 scores had also decreased, from 31.4±9.1 to 29.6±10.9 (paired t-test, p=0.02), and MMSE score had increased from 20.7±4.2 to 21.6±4.9 (paired t-test, p<0.01). However, DAD-K (86.5±18.3 to 88.4±17.4), S-IADL (14.1±10.4 to 12.9±10.5), and CDR (4.5±3.0 to 4.4±3.1) scores did not change significantly during the trial period.
Correlation analyses between changes in choice or simple reaction times and measurements of cognition and ADL are presented in Table 3. Although there were significant improvements in attention measures over the 12-week trial period, no significant correlation was observed in the current analyses. The differences in simple and choice reaction times over the trial period were not significantly correlated with changes in either cognition or ADL.
The PP groups were stratified into quartiles according to improvements in choice or simple reaction times at 4 weeks after study enrollment in order to explore whether the improved global function observed following galantamine therapy was attributable to the galantamine-induced improvement in attention function (Table 4). These responder analyses also did not detect any significant association between improved attention function at week 4 and the prevalence of responders in cognition and ADL measures.
Discussion
This was a single-arm, multicenter, prospective study investigating the effect of galantamine on attention function in AD patients. We found a significant improvement in attention starting as early as 4 weeks after the commencement of galantamine therapy in patients with mild to moderate AD, and a persistent improvement in attention as late as 12 weeks, as reflected by changes in simple and choice reaction times, in agreement with previous reports.15,16 Attention is increasingly recognized as an important factor affecting cognition and ADL. It can be further broken down into selective attention, sustained attention, and divided attention. Decreased cholinergic and nicotinic signaling was postulated to contribute to attention deficit in AD patients, and it is believed that nicotinic augmentation is associated with increased attention function.17 Galantamine enhances neurotransmission through its antiacetylcholinesterase activity, and plays a role in nicotinic receptor modulation via allosteric potentiation.18,19 It has been shown that there is a correlation between the number of nicotinic receptors and attentional function in AD patients.20
However, we found no association between improved attention function resulting from taking galantamine for over 12 weeks and longitudinal changes in cognition and ADL in these AD patients. Attention is a basic component of cognition and allows other cognitive domains to function properly.20 Therefore, current measures of global functioning such as ADAS-cog11, DAD-K, and S-IADL would not be directly related to attention function, since many other cognitive domains are involved between attention and cognition/ADL. In other words, the level of attention function required in everyday life is not high, so that such measures of cognition and ADL are not suitable for linking attention functions. In this context, more specific and elaborate measurement tools for assessing daily lives are warranted to prove our original hypothesis that improved attention function by galantamine benefits cognition and ADL.
We employed computer-based tests to capture any change in attention pre- and postgalantamine treatment that would otherwise not be detected with traditional pencil-and-paper tests. We developed our own computer program that was designed to not only measure simple and complex reaction times, but also assess divided attention. However, despite the demonstration of improvement in attention in general, neither simple attention nor the complex attention functions exhibited any significant correlation with cognitive and functional improvements in AD patients receiving galantamine. The difference between simple and choice reaction times can be interpreted as mental processing involving the cognitive response to the stimulus. This could be another way to look at the possible relationship between attention/working memory and global function. We analyzed this possible relationship, and did not find it to be statistically significant. ADAS-cog11 and S-IADL certainly require some attention to be completed successfully, but do not necessarily mandate fast reactions nor divided attention. This may well explain why those tests yielded no correlations.
This study was subject to several limitations that should be taken into account when interpreting the results. The sample was too small to reveal differences. There were many dropouts due to protocol deviations during the course of the study. In addition, Korean elderly subjects are generally uncomfortable with computer-based tests because many of them have a low educational attainment and are not used to interacting with computers. This might have hampered the detection of changes in attention. Furthermore, the study duration of 12 weeks may have been too short to observe any meaningful changes in the attention and global function of these AD patients. Due to time and budget constraints, the computer program used to measure attention, and particularly divided attention, was not first pilot-tested on an AD population and normal controls, and hence its validity in patients with AD remains unclear. Finally, this study was limited by its open-label design and lack of a placebo arm. The lack of a placebo makes it difficult to accurately interpret the analyzed data. We attempted to minimize these limitations by blinding the raters to the outcome measures.
Further larger studies with longer intervention periods are warranted to confirm the relationship between attention and global functioning. To move forward, it may be necessary to design a study using neuroimaging that can decisively elucidate the relationship between attentional function and cognition or ADL.





 XML Download
XML Download