

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sleep-state misperception, which is also known as subjective insomnia and paradoxical insomnia, is considered a subtype of primary insomnia,12 and describes people who mistakenly underestimate their total sleep time (TST) relative to the normal TST, as assessed using objective studies such as polysomnography (PSG) or actigraphy. Although no large-scale, community-based studies have investigated the prevalence of sleep-state misperception and its variable definitions, some studies have investigated the prevalence of this disorder, and found it to be 9.2-50%.3456789 These prevalence studies suggest that sleep-state misperception is a relatively common condition among primary insomnia sufferers.
Insomnia is a common complaint in Korean adults, with about 22.8% reportedly suffering from primary insomnia, a rate that is similar to that reported for Western countries.10 However, to the best of our knowledge there have been no studies on the prevalence of sleep-state misperception and its associated factors in Asian adults.
The purpose of this study was to identify the prevalence of sleep-state misperception in primary insomnia sufferers and to assess the clinical predictors of this disorder in primary insomniacs.
METHODS
Subjects
Two hundred and fifty primary insomnia patients who visited a regional sleep center between April 2009 and October 2013 were retrospectively selected from a sleep center registry. Primary insomnia was diagnosed according to the fourth edition of the Diagnostic and Statistical Manual, text revision.11 All subjects who were selected in our study were older than 18 years and had an objective TST of >120 min. Patients with other comorbid sleep disorders such as obstructive sleep apnea and restless legs syndrome were excluded, as were those who did not complete a full-night PSG, self-reported questionnaire, or interview regarding subjectively estimated TST the morning after the PSG. Insomniacs who answered that the previous night's sleep differed from their usual sleep experience were also excluded. The selected patients were divided into two groups according to the presence or absence of sleep-state misperception, which was defined according to the research criteria for paradoxical insomnia, by an objective TST of at least 6.5 h and an objective sleep efficiency (SE) of at least 85%.12
Ethical approval for this study was obtained from the local institutional review board.
Full-night PSG
A full-night PSG consists of continuous recordings from six electroencephalogram leads (C3-A2, C4-A1, F3-A2, F4-A1, O1-A2, and O2-A1 in the international 10-20 system), two electro-oculogram leads (ROC-A1 and LOC-A2), and three electromyogram leads (submental and bilateral tibialis anterior). The equipment includes thermistors for measuring the temperatures of the nasal and oral airflows, an airflow pressure transducer for measuring nasal air pressure, a microphone for snore detection, strain gauges for measuring thoracic and abdominal excursion, finger pulse oximetry, and electrocardiogram leads. Each epoch is staged and scored according to the international criteria of the 2007 manual from the American Academy of Sleep Medicine.13
Subjective measures
Before the full-night PSG study, all of the subjects completed the self-reported questionnaires with demographic factors, health/medical history, sleep-related scales, and psychiatric measurements including the Korean versions of the Insomnia Severity Index (K-ISI),14 Pittsburgh Sleep Quality Index (K-PSQI),15 Epworth Sleepiness Scale (K-ESS),16 Beck Depression Inventory-2 (K-BDI-2),17 Hospital Anxiety and Depression Scale,18 and Short-Form 36-Item Health Survey.19
In the morning after a full-night PSG, all subjects were interviewed by a PSG technician. Their TST of the previous night was estimated by the hour and they were asked whether they thought it had been an ordinary night. The sleep estimation error was calculated by subtracting the objective TST from the subjective TST (PSG) values.
Statistical analysis
The data analyses were performed using SPSS version 18.0, and the threshold for statistical significance was set at p<0.05. Descriptive statistics were used to examine the demographic data. Analysis of covariance (ANCOVA) was used to analyze sleep- and psychiatric-related characteristics, and for some of the PSG variables. The factors related to subjective TST and sleep quality were analyzed using stepwise regression. Except where stated otherwise, the data are presented as mean±SD values.
RESULTS
Among 250 primary insomniacs, 66 (26.4%) were classified as having sleep-state misperception; their demographic and clinical characteristics are listed in Table 1. The patients with misperception were significantly younger than those without misperception (47.48±12.63 years vs. 54.24±11.32 years, p<0.001). There were no significant differences between the two groups with respect to other variables such as gender, body mass index, and underlying diseases.
The PSG data of the patients with and without misperception groups are listed in Table 2. The misperception group exhibited relatively normal sleep architecture; their total recording times (470.56±21.42 min vs. 457.00±24.22 min, p<0.001) and TST (422.80±22.67 min vs. 304.38±66.73 min, p<0.001) were significantly longer than in those without misperception, and their latency to sleep onset (6.94±4.78 min vs. 24.54±25.02 min, p<0.001) and latency to rapid eye movement sleep (REM; 90.40±47.79 min vs. 131.25±82.93 min, p<0.001) were significantly shorter. The misperception group had a shorter wake-after-sleep onset time (40.82± 13.64 min vs. 128.07±55.97 min, p<0.001) and better SE (89.25±2.80% vs. 66.55±14.08%, p<0.001). Furthermore, the misperception group had a nearly normal sleep architecture, while those without misperception had a shorter REM sleep time relative to TST (17.29±7.87%, p<0.001) and a longer light sleep time (N1+N2 stage) relative to TST (62.42±13.3%, p=0.006).
The subjective TST was 233.55 min in those with misperception and 147.93 min in those without misperception (Table 3). While a tendency toward underestimation of subjective TST was apparent in both groups, the sleep estimation error (subjective TST minus objective TST) was significantly greater in those with misperception than in those without misperception (-189.25±91.29 min vs. -156.45±11.32 min, p=0.009).
The results of the subjective measures are listed in Table 4. In terms of sleep-related measures, including K-ISI, K-PSQI, and K-ESS scores, there were no significant differences between those with and without misperception. Although K-ESS scores were within the normal limits, the K-ISI scores revealed moderate insomnia in both groups (21.64±4.67 vs. 21.70±4.84), and the total K-PSQI score revealed poor sleep quality in both groups (14.38±3.26 vs. 15.19±2.93). The psychiatric variables did not differ significantly between the two groups, with both groups demonstrating a moderate depressive mood, anxiety, and poor quality of life.
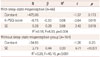
Multivariate analysis was used to determine the factors affecting subjective TST and subjective sleep quality. In both groups, the objective SE, as calculated from the PSG, was a significant factor associated with subjective TST (Table 5). However, the effect size was greater among those without misperception than among those with misperception. In the misperception group the total K-PSQI score was also significantly associated with subjective TST, the effect size being the same as that for objective SE. In terms of subjective sleep quality, the subjective TST was a significant factor related to K-PSQI score in the misperception group, while the K-BDI-2 score and age were significant effect factors in those without misperception (Table 6).
DISCUSSION
The prevalence of sleep-state misperception among the adult primary insomniacs in the present study was 26.4%, suggesting that this condition is not uncommon among Korean primary insomniacs. This prevalence was lower than reported previously (34.4-50%),3456789 which may be at least partly attributable to racial differences between the study populations, and to variations in the definition of sleep-state misperception used and efforts to eliminate the first-night effect of PSG.
Patients with sleep-state misperception were younger than those without misperception. The findings regarding the influence of age in sleep-state misperception are inconsistent.352021 Most studies have found age to not be a significant factor;320 we found only one report of an age difference between patients with and without misperception.21 However, the definition of sleep-state misperception differed between that study and the present study. Although it is possible that age is an influencing factor in sleep-state perception, further study is required to confirm the present finding in this regard and to establish the underlying mechanism.
The objective parameters obtained from a full-night PSG were significantly better in those with misperception than in those without misperception. Primary insomniacs with sleep-state misperception exhibited a nearly normal sleep structure on the full-night PSG. This finding is consistent with those of previous studies.2612 One study that applied power spectral analysis to EEG recordings found that patients with sleep-state misperception had a lower relative activity in the slower frequency bands in REM compared with healthy sleepers.20 Further studies with new methodologies, rather than routine PSG, are required to determine the possible objective difference in sleep compared with normal sleepers and the mechanism underlying sleep-state misperception.
The subjective measures, including sleep-related and psychiatric variables, did not differ between those with and without sleep-state misperception. Despite their better full-night PSG results, primary insomnia sufferers with misperception complained of moderate insomnia, poor subjective sleep quality, moderate depressive mood/anxiety, and poor health-related quality of life to a similar degree to primary insomniacs without misperception. This suggests that all patients with insomnia, both with and without misperception, need active treatment for their insomnia symptom and related psychiatric symptoms, despite the better normal PSG results in the former group. Furthermore, the goal of treatment for primary insomnia with misperception should not be the normalization of the objective sleep structure.
While both groups underestimated their subjective TST compared to their objective TST, the sleep estimation error was significantly larger in the misperception group. According to some early studies of sleep-state misperception, underestimation of subjective TST and overestimation of sleep difficulty is a common tendency among primary insomnia sufferers.2223 However, more recent studies suggest that sleep-state misperception is variable across primary insomnia sufferers.2425 The sleep estimation error differed significantly between those with and without misperception in the present study, suggesting that the underestimation of TST is a defining feature of the subgroups of primary insomnia with misperception.
The SE of a full-night PSG was significantly associated with subjective TST in both groups in this study; however, the multivariate effect size was larger among those without misperception (R2, 0.20 vs. 0.07). Moreover, the total K-PSQI score was related to subjective TST only in the misperception group. These data further support the suggestion that sleep-state misperception is a discrete subgroup of primary insomnia. Age, psychiatric variables including anxiety and depression scale scores, and PSG variables other than SE were not associated with subjective TST in either group.
A particularly interesting finding was that the factors affecting subjective sleep quality as measured by K-PSQI score differed between the groups. In the group with misperception, subjective TST was found to be associated with K-PSQI score, in those without misperception, K-BDI-2 score and age were the associated factors. This finding suggests that these two groups are indeed different, and that the treatment goal should therefore differ between these groups. In particular, the treatment goal of insomnia sufferers with misperception should include correcting their underestimated subjective TST. Cognitive behavioral therapy (CBT) may be effective in this regard, as supported by one study finding that CBT can change the discrepancy between subjective and objective measures in older adults with comorbid insomnia.26 Further study is needed to elucidate the effectiveness of CBT for the misperception subgroup of primary insomnia sufferers.
This is the largest study of Korean adult primary insomnia sufferers with sleep-state misperception to date. The objective PSG data and subjective measures including sleep-related questionnaire scores and psychiatric measures were analyzed. However, the findings of this study should be considered in the light of certain limitations. First, the insomnia patients were asked one simple question about subjective TST rather than gathering detailed sleep diaries from them, and so only subjective TST could be calculated, despite the measurement of other parameters such as subjective sleep latency, which are also important for defining sleep-state misperception. Second, only a single full-night PSG was performed; the first-night effect was not fully excluded, although patients who answered that their sleep during the PSG was not the same as their usual sleep experience were removed from the analysis. Third, this study was performed at a single tertiary center, and a full-night PSG study is relatively expensive in Korea. It is therefore possible that the study sample is not representative of the general population. Finally, the retrospective design of this study limits the power of its findings.
In conclusion, the patients with sleep-state misperception had greater subjective complaints of insomnia, poorer quality of sleep, and more abnormal psychiatric measurements in comparison with the norm. These symptoms were similar to those with primary insomniacs without misperception. However, the objective PSG data and the factors affecting subjective TST and sleep quality differed between the two groups, suggesting that these two groups should be separated and their treatment goals should be different.





 XML Download
XML Download