

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A wide variety of factors influence stroke prognosis, including stroke severity, location, and mechanism, comorbidities, clinical findings, and age. Interventions such as care in stroke unit or intensive care unit (ICU) and rehabilitation can also play important roles in stroke outcome.1234 Knowledge of the important factors that affect prognosis after stroke is essential for an integrated approach for the treatment of stroke patients in the acute phase, and to enable an accurate prognostic prediction for individual patients.
Lateral medullary infarction (LMI) is a vascular disease of the brainstem, and atherosclerosis of the vertebral artery (VA) or posterior inferior cerebellar artery (PICA) is the most common cause (50%). Dissection of the VA or PICA, small vessel occlusion (SVO) (13%), and cardioembolism (5%) are other etiologies.5 Previous studies have shown that most patients with LMI have a good prognosis. However, there have been a few reports on the influence of lesional differences on complications including severe dysphagia and aspiration pneumonia, which are common in large and rostral lesions, although the clinical localization and the correlation on magnetic resonance imaging (MRI) may sometimes be inconsistent.678910 There remains a paucity of data about the long-term prognostic factors and complications associated with acute LMI.911 Therefore, the aim of this study was to identify independent predictors of poor outcome after acute LMI based on experiences at a single center over 11 years.
METHODS
Study population
Initially, 8,437 patient records were screened via a search of the electronic medical records of patients who were hospitalized at our institution over an 11-year period between February 1, 2004 and November 31, 2013, and then followed up until November 31, 2014. In total, there were 157 patients with acute ischemic stroke (IS) involving a lateral medullary lesion, as identified on brain MRI scans within 7 days after stroke onset. All patients were at least 18 years of age (range, 30-91 years) and were followed up at our hospital during the study period. Patients whose brain MRI and conventional angiography were limited to evaluation of LMI lesions and arterial lesions, and for whom there was a lack of medical and clinical information and no outcome data, were excluded from the study. The baseline characteristics did not differ significantly between the study patients and those who were excluded (supplementary data). This study was approved by the Institutional Review Board of our medical institution. The requirement for informed consent was waived due to the retrospective nature of this study.
Baseline and clinical assessment
Baseline characteristics such as demographic data (age and sex) and conventional vascular risk factors [hypertension, diabetes mellitus, a past history of smoking, hyperlipidemia, heart disease, and a past history of stroke/transient ischemic attack (TIA)] were evaluated. Several laboratory findings related to inflammation, such as white blood cell (WBC) count, and serum concentrations of glucose and C-reactive protein (CRP), were also evaluated using routine laboratory methods. Blood samples were withdrawn after overnight fasting. The following definitions were used for clinical assessments:
1) Hypertension: a history of antihypertensive treatment, a systolic blood pressure of ≥140 mm Hg, or a diastolic blood pressure of ≥90 mm Hg.12
2) Hyperlipidemia: a history of antihyperlipidemia medication or a serum level of total cholesterol of >6.2 mmol/L (240 mg/dL).13
3) Diabetes mellitus: glycated hemoglobin (HbA1c) of ≥6.5%, fasting blood glucose of ≥126 mg/dL, or nonfasting blood glucose of ≥200 mg/dL, or the use of insulin or oral hypoglycemic drugs.14
4) Heart diseases: including arrhythmia, coronary artery disease, congestive heart failure, and valvular heart diseases.
5) Smoking: indicated if a patient was either a current smoker or an ex-smoker.
Neurological assessment
All of the patients were initially evaluated for stroke severity based on the National Institutes of Health Stroke Scale (NIHSS) neurological examinations, including sensory symptoms and ataxia, for which the functional status was evaluated by board-certified experts in neurology at the outpatient clinic or through a structured telephone interview by a trained nurse at 3 months and 1 year poststroke. These evaluations represented attempts to monitor the quality of inpatient stroke care. Initial dysphagia was identified based on electronic medical records using the initial bedside swallowing tests, evaluated by trained physicians within 1 day after admission to the hospital. This test included an evaluation of the level of consciousness, deglutition, voice change, evidence of coughing, drooling, oral motor control, control of bolus in the oral phase, and evidence of delay in the swallowing reflex. The patients were then managed by diet modification and swallowing therapy.1516
Functional outcomes were evaluated using the modified Rankin Scale (mRS), the scores for which were used to divide the patients into two groups: favorable outcome (mRS score ≤1) and unfavorable outcome (mRS score ≥2).17 The occurrence of clinical events during a 1-year period since the onset of LMI was evaluated; these events included IS, TIA, myocardial infarction, pneumonia, ICU treatment, and death. The following definitions were used:
1) IS: the presence of findings suggestive of stroke with a duration of ≥24 hours, or MRI-confirmed acute IS with a duration of <24 hours.
2) TIA: Acute loss of focal neurological signs of vascular origin, accompanied by the resolution of symptoms within 24 hours.
3) Death: sudden death occurring within a 1-year period since the onset of LMI as a result of vascular or nonvascular events due to underlying conditions such as cancer, pneumonia, or respiratory failure.
4) Pneumonia: radiologic evidence of consolidation or infiltration and at least one of the following conditions: granulocytosis, fever of >38℃ and/or cough, sputum, and shortness of breath.18
Based on the Trial of Org 10172 in Acute Stroke Treatment criteria and arterial dissection alone, cases of stroke were categorized as follows:19202122 1) large-artery atherosclerosis (LAA), 2) SVO (hypertension, no cardioembolic source and normal angiography), 3) cardioembolism, and 4) VA or PICA dissection.
Evaluation of LMI on brain MRI and conventional angiography
Brain MRI/MR angiography (MRA) and conventional angiography were used to assess the LMI lesion and dissection of the VA and PICA. Brain MRI/MRA was performed using a 1.5-T or 3.0-T superconducting magnet system. VA or PICA dissections were defined as images of a 'double lumen,' 'intimal flap,' 'string-of-pearls appearance,' 'steno-occlusion,' and 'fusiform aneurysmal dilatation' on either brain MRI/MRA or conventional angiography.22 Based on previous reports, the LMI lesions were classified into three categories: rostral, middle, and caudal (Fig. 1).523 Two board-certified experts in neurology who were blinded to the clinical characteristics retrospectively reviewed and classified the findings on brain MRI/MRA and conventional angiography.
Statistical analysis
Student's t-test and Pearson's χ2 test were used to compare differences in continuous and categorical variables, respectively, between the two groups. Multiple logistic regression analysis was also performed to identify correlations between age, conventional vascular risk factors, initial symptoms, and the pathophysiology of stroke, and functional outcomes using statistically significant variables (p<0.05). In addition, odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by adjusting those variables known to have a correlation with functional outcomes, including patient age, conventional vascular risk factors, initial symptoms, clinical complications, pathophysiology of the stroke, laboratory finding such as WBC count, serum CRP, and LMI lesions. All the tests were two-sided, and the threshold of statistical significance was set at p<0.05. All statistical analyses were conducted using SPSS software (Version 21.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
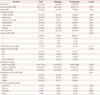
In total, 157 patients with acute LMI were enrolled; these patients were aged 60.1±12.3 years (mean±SD; range, 30-91 years) and showed a male predilection (73.2%). The demographic characteristics, conventional vascular risk factors, initial clinical symptoms, laboratory findings, and types of stroke are presented in Table 1 relative to functional outcome at 1 year. Of the 157 patients, 93 (59.2%) had favorable outcome and 64 (40.8%) had an unfavorable outcome. The mean age was significantly higher in the unfavorable outcome group than in the favorable outcome group (p=0.003), as were the prevalence rates of hypertension and hyperlipidemia (p=0.008 and p<0.001, respectively). The NIHSS score did not differ significantly between the two groups [mean, 2 (range 1-3) vs. 2 (range 1-4); p=0.437]. The most common type of stroke was LAA in both groups (61.3% and 62.5%, for the favorable and unfavorable outcome groups, respectively). The prevalence of cardioembolism was significantly higher in the unfavorable outcome group than in the unfavorable outcome group, whereas that of SVO was significantly higher in the latter (p=0.016) (Table 1). At 1 year after LMI onset, five patients had suffered a stroke/TIA arising from LAA (data not shown). The serum level of CRP was significantly higher in the unfavorable outcome group than in the favorable outcome group (p=0.036).
Clinical features and outcome according to initial clinical symptoms
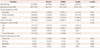
The prevalence of dysphagia at the time of stroke was significantly higher in the unfavorable outcome group (p=0.017) (Table 1); however, the prevalence rates of sensory symptoms and ataxia did not differ significantly between the two groups (Table 1). The baseline characteristics, stroke types, and outcome are presented in Table 2 relative to the presence of dysphagia. None of the baseline characteristics or conventional risk factors differed significantly between those with and without dysphagia, and LAA was the most common stroke type in both groups. Cardioembolism was significantly more common among those with dysphagia, whereas SVO was significantly more common among those without dysphagia (p=0.006) (Table 2).
The mortality and prevalence of pneumonia appeared to be higher among those with dysphagia, but the difference was not statistically significant (p=0.190 and 0.423, respectively). However, the serum level of CRP, WBC count, and frequency of an unfavorable prognosis were all significantly higher among those with dysphagia than among those without dysphagia (p=0.004, 0.028, and 0.017, respectively) (Table 2).
Clinical features and outcome according to LMI lesion characteristics
The clinical symptoms/signs and prognosis relative to the lesion type are presented in Table 3. Although dysphagia appeared to be more prevalent in the middle medulla, the difference was not statistically significant (p=0.061); however, sensory symptoms were significantly more prevalent in the caudal region (p=0.026). In addition, LAA was the most common of all of the LMI lesions (p=0.143). Cardioembolism was the most common LMI lesion in the rostral region (16.7%, 5.3%, and 0% in the rostral, middle, and caudal regions, respectively).
There was a nonsignificant tendency toward a greater rate of stroke/TIA recurrence and pneumonia with rostral medulla LMIs (p=0.665 and 0.557, respectively). However, ICU treatment and mortality were encountered significantly more frequently among patients with LMIs in the rostral region as compared with the other two regions (p=0.002 and 0.002, respectively). The rostral medulla tended to be a less common LMI location than either the middle or caudal medullae in the favorable outcome group, but again the differences did not reach statistical significance (p=0.135 and 0.186, respectively) (Table 3).
Clinical complications and prognosis at 1 year
At 1 year post-LMI, the frequencies of pneumonia and ICU treatment were significantly higher in the unfavorable outcome group than in the favorable outcome group (p=0.025 and 0.001, respectively) (Table 1). Seven of the patients died of medical conditions such as septic shock and underlying critical diseases (gastric cancer and hematologic cancer); there were no cardiovascular deaths (Table 1). The mean age was significantly lower in the favorable outcome group than in the unfavorable outcome group (57.7±11.0 years vs. 63.6±13.4 years, p=0.003).
The impact of several factors on functional outcome at 1 year was investigated. Conditional logistic regression analysis revealed that older age and initial dysphagia were independently associated with unfavorable outcome at 1 year (older age: OR=1.04, 95% CI=1.001-1.087, p=0.049; initial dysphagia: OR=2.46, 95% CI=1.04-5.84, p=0.041). In addition, hyperlipidemia had a profound impact in the unfavorable outcome group compared to the other variables (Table 4).
DISCUSSION
The results of this study show that initial dysphagia is an important factor associated with poor outcome at 1 year after LMI. Furthermore, consistent with previous reports, older age was also an independent variable with predictive value for a poor prognosis at 1 year after LMI.242526 It has been reported previously that dysphagia is a common consequence of medullary infarction, but often improves rapidly so that patients can return to oral feeding within 1-2 months after stroke.27 However, the recovery from dysphagia in some patients is rather slow, and severe dysphagia is associated with hospital mortality rates of 2.9-11.6%, and pneumonia.79101128 A few studies have found increased mortality and a poor functional outcome in patients with clinically apparent dysphagia after hemispheric stroke.2930 In these cases the severity of the dysphagia after LMI is greater than in patients with unilateral hemispheric stroke due to 9th and 10th cranial nerve involvement. Although a medullary lesion is unilateral, its effect on swallowing is bilateral.10 The incidence of pneumonia among patients with dysphagia has been reported to lie in the range 7-29%.31 The incidence of pneumonia is more strongly associated stroke with dysphagia than stroke without dysphagia.1011
In this study the proportion of the present LMI patients with dysphagia was 34%, which is lower than those reported previously (51-94%).7 The difference in the incidence of dysphagia between these studies may be attributable to the inclusion in the present study of patients with a positive objective screening test. In much of the literature, dysphagia has been poorly classified, videofluoroscopy was only rarely used, and the definitions of dysphagia are unclear.28 Dysphagia was defined herein after a positive dysphagia test applied by a trained physician; that test was previously demonstrated to be reliable for detecting dysphagia.32
In the LMI patients, dysphagia was more frequently observed with deep lesions than with superficial lesions. Examination of the correlation between the complications of LMI and the vertical location of lesions on brain MRI has revealed an association between rostral and middle lesions of the medulla, and the occurrence of dysphagia and pneumonia in these patients. In this study the frequency of dysphagia was lower in the rostral medulla as compared with previous studies, because more of the patients with LMI had middle lesions compared with previous studies.2328 The main swallowing centers of the nucleus tractus solitarius, nucleus ambiguous, and reticular formation are involved in deep lesions of the dorsolateral medulla.
This study found that the frequencies of aspiration pneumonia and ICU treatment were significantly higher in the unfavorable outcome group than in those with a good outcome after LMI. In addition, although not statistically significant, there was a tendency toward a higher frequency of death, pneumonia, and ICU treatment among those with dysphagia compared to those without following LMI. These complications and dysphagia were associated with rostral and medullary LMI lesions. The rates of mortality and ICU treatment were higher for those with rostral medulla LMIs as compared with other lesions, indicating that complications in those with rostral LMI lesions may be associated with the severity of dysphagia.101127 In addition, prolonged dysphagia might predispose patients to malnutrition, which is related to a poor outcome after stroke.3033
It has been reported that younger age is significantly correlated with a favorable outcome and various pathophysiologies of stroke, with younger patients being more likely to make a full recovery from IS than are their older counterparts.242526 According to animal studies, aged rats exhibited premature scar formation and delayed neuron regenerative capacity in the brain due to impaired glial repair, angiogenesis, and neuronal regulation.3435
LAA was the most common stroke etiology, regardless of the outcome, and SVO was more common in the favorable outcome group than in the unfavorable outcome group, as reported previously.13 With regard to the correlation between the degree of neurological recovery and the pathophysiology of LMI, patients with SVO had better outcomes, while initial stroke severity was similar in both groups. This finding could be associated with the apparently lower frequency of dysphagia in the SVO group (Table 2); however, this association did not reach statistical significance on multiple logistic regression analysis (p=0.059).
The findings of this study should be considered in light of several limitations:
1) Its retrospective design, which raises the possibility of bias with respect to review of the demographic, epidemiologic, and clinical data of the patient series.
2) The lack of data regarding the correlations between the prognosis and the severity of dysphagia, as assessed using videofluoroscopy. Moreover, no data on the duration of dysphagia after acute LMI are presented.
3) The severity of sensory symptoms and ataxia were not reviewed at 1 year. The reason for this was that mRS is commonly used to evaluate the degree of disability or dependence in daily activities after the onset of stroke or other causes of neurological disability.
4) Only a small number of patients were enrolled in the current study, although the study population was larger than in previous related studies. The results therefore cannot be generalized, and so further large-scale, multicenter studies are warranted to confirm the correlations between prognosis or etiologic factors and LMI demonstrated herein.
In conclusion, initial dysphagia and older age appear to be independent predictors of poor outcome after LMI, and the application intensive medical care was associated with a reduction in the incidence of pneumonia. Intensive treatment for dysphagia is recommended in both young and old patients after LMI for appropriate nutritional support, in order to prevent aspiration and a poor prognosis. Prevention of aspiration due to dysphagia and improving nutritional condition in patients with LMI may improve the patient's functional outcome and quality of life.



 XML Download
XML Download