

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Posterior reversible encephalopathy syndrome (PRES) refers to a clinicoradiological entity with characteristic features on neuroimaging and nonspecific symptoms comprising headache, confusion, visual disturbances, and seizures. This syndrome may occur in diverse situations, including the taking of cytotoxic and immunosuppressive drugs, hypertensive encephalopathy, and eclampsia. The lesions in PRES are thought to be due to vasogenic edema that occurs predominantly in the posterior cerebral hemispheres, and are reversible with appropriate management. We present herein the case of a female with sickle cell (SC) disease who presented with this syndrome without any of the common risk factors.
A 57-year-old woman presented to the emergency room with confusion and behavioral changes of sudden onset. Her medical history included a SC disease and supraventricular tachycardia for which she was being treated with flecainide, atenolol, and aspirine.
On the day before admission, the patient presented with a SC vaso-occlusive crisis with diffuse pain in both lower limbs. The examination upon admission revealed confusion, temporo-spatial disorientation, behavioral disorders, dysarthria, phasic disorders, a discrete right motor deficit, and psycho-motor slowing. She complained of leg pain, her blood pressure was 139/89 mm Hg, and there was no fever.
Laboratory tests revealed normal renal function and serum electrolytes, but impaired liver function. Her hemoglobin and platelet count were 8.8 g/dL and 74,000/mm3, respectively, and her white blood cell count was elevated at 11,000/mm3. Lumbar puncture findings were normal; blood, urine cultures, and serology tests (HIV, human T-lymphotropic virus, syphilis, herpes, hepatitis C, leptospirosis, Lyme) produced negative results, hepatitis B, cytomegalovirus and Epstein-Barr virus serologies were in favor past healed infections.
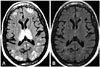
Brain MRI revealed multiple bithalamic, biparietal, bitemporal, bifrontal, and cerebellar subcortical high signal intensity lesions on T2-weighted, fluid-attenuated inversion recovery and diffusion-weighted sequences (Fig. 1A). Apparent diffusion coefficient mapping revealed a high signal indicative of the presence of vasogenic edema. Control MRI performed after 15 days revealed complete resolution of the bithalamic lesions and all other lesions (Fig. 1B). The patient's clinical status also normalized spontaneously.
The case described herein is thus far unique in that while lesions in PRES usually involve mainly the parieto-occipital lobes, in this case the lesions also involved both thalami, the cerebellum, and the temporal and frontal lobes. The diagnosis of PRES was confirmed by the radiological features disappearing at follow-up MRI performed 15 days later. The originality of this case also lies in the very rare cases of PRES described in SC patients being associated with severe acute chest syndrome, uncontrolled hypertension, renal failure, or pulmonary infection,123 which was not the case in the present patient. In those previously described cases, PRES was attributed to abrupt elevation of blood pressure, or blood volume. It is possible that our patient presented with relative hypertension, since SC patients generally have a lower blood pressure than non-SC controls.
Reversible posterior leukoencephalopathy syndrome (RPLS) was described by Hinchey et al.4 in patients with hypertension, eclampsia, renal failure, or with immunosuppressor treatments. The syndrome includes headache, transient neurological symptoms, visual changes, seizures, or altered consciousness, with MRI revealing subcortical edema in the posterior regions of the cerebral hemispheres without infarction; these clinical and radiological findings are reversible with control of blood pressure or withdrawal of immunosuppressive therapy. Since the gray matter can also be involved, the term RPLS has been replaced by PRES.
The pathophysiology of PRES remains a matter of debate. One hypothesis is that severe hypertension in these patients causes impaired cerebrovascular autoregulation, vasodilatation, and vasogenic edema, while another is that toxicity of immunosuppressive drugs (e.g., tacrolimus or cyclosporine) leads to impaired endothelial homeostasis. However, PRES appears ultimately to be related to endothelial dysfunction that leads to cerebro-vascular autoregulation impairment and vasogenic edema.2 Since endothelial dysfunction is thought to play part in the cerebrovascular disease observed in SC anemia, SC patients may have an increased risk of developing PRES.2
In addition to more classical neurological complications of SC disease, such as ischemic strokes, silent cerebral infarcts, intracerebral hemorrhages or seizures, PRES may also be evoked in patients presenting with acute neurological changes, even in the absence of risk factors, as in our case.
 XML Download
XML Download