

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cysticercosis is a zoonosis caused by the encysted larval stage of the tapeworm Taenia solium. Cysticercus refers to the resting stage of the larva of the cestodes. It can affect any organ of the body, but the cerebral parenchyma is the most common site in the central nervous system (CNS; 60-90%), where it causes neurocysticercosis. Neurocysticercosis is one of the most common helminthic human infestations of the CNS1 and is one of the most common causes of acquired seizures in endemic countries.2 Cysticercosis is highly endemic in most developing countries because of poor socioeconomic development.3 About 50 million people in the world today are infected by the taeniasis-cysticercosis complex, and 50,000 of those die every year as a result.4 Human infestation develops after the ingestion of eggs from the feces of a tapeworm carrier (i.e., fecal-oral contamination) or consumption of meat from an intermediate host.5 In the brain, it occurs in two forms: parenchymal and extraparenchymal or racemose cysts. The clinical presentation of racemose cysts is pleomorphic, and quite different from parenchymal cysticercosis.
LIFE CYCLE AND PATHOGENESIS
Humans are the only definite hosts for T. solium, while pigs act as the intermediate hosts. Humans can also act as intermediate hosts after consumption of T. solium eggs. In the intermediate host, it transforms into a "bladder worm" composed of a vesicle with a central fluid-containing cavity and an invaginated scolex on its wall. In the human host, adult tapeworms develop in the intestine after ingesting cysticercus in undercooked pork. These adult tapeworms shed proglottids, with each proglottid containing 1,000-2,000 eggs. The oncospheres hatch in the intestine and then penetrate the intestinal wall before disseminating to various body tissues including the CNS to form cysticerci. The cysticerci in the brain undergo four stages of involution.6 Stage one is the vesicular stage, which is characterized by a cyst with a vesicular, translucent wall with transparent fluid and a viable invaginated scolex. This stage is followed by the colloidal stage, which is characterized by a cyst with a thick wall, turbid fluid, and a degenerating scolex and induces a host inflammatory response. The cyst subsequently degenerates as it moves into the granular stage, which is characterized by a cyst with a thicker wall, degenerated scolex, and little associated inflammatory response. Finally, the cyst transforms into a coarse calcified nodule (calcific stage).
There are several types of neurocysticercosis lesion based on the location of the parasite in the CNS. They frequently present as focal lesions in the brain parenchyma with surrounding edema, which subsequently undergo calcification. The most frequent CNS location is in the cerebral hemispheres, commonly at the junction between the gray and white matters.7 Cysticercosis in a cerebellar location is rare, but there have been a few case reports.89 The rarity of cysticercosis in the cerebellum may be attributable to its less-abundant blood flow relative to the cerebrum.
Other extraparenchymal CNS sites include the ventricles, cisternal/subarachnoid spaces, spinal cord, and ocular bulb.10 Many patients may have a combination of these types. Cysts in a subarachnoid location are less common and occur in the basal cisterns or Sylvian fissures. Macroscopically, they appear like a cluster of grapes and are termed a racemose variety of neurocysticercosis.11 Racemose neurocysticercosiss differ from parenchymal lesions in several ways, and are referred to as "aberrant proliferating cestode larvae." They arise from segmentation of cysticercosis cellulosae with sprouting of new cysts. These new cysts gradually expand with degeneration of the scolex and are nonviable and degenerated interconnected bladders of various sizes.12 They are seen as abnormal growths of cystic membranes without a scolex that occur in and around the brain in areas such as the suprasellar, Sylvian, and quadrigeminal cisterns. They are larger because in the cisternal or subarachnoid space there is no limiting parenchymal tissue that can act as a host response for encapsulation. The size of racemose neurocysticercosises varies from 4 to 12 cm,13 and they are identified on magnetic resonance (MR) imaging (MRI) as multiple cystic lesions.
The usual temporal development of the degenerative stages as seen in the aforementioned parenchymal types is lacking in racemose types,14 and the scolices on its wall are absent in most racemose cases (Fig. 1).15 Racemose cysticercus may be due to a different variety of cestode, which could be either an aberrant cysticercus of T. solium or a sterile coenurus of Taenia multiceps or Taenia serialis.16 It is clinically more aggressive than the parenchymatous form and is reportedly seen in 15-54% of patients.17181920 Racemose neurocysticercosises are considered as malignant forms of neurocysticercosis if they are associated with hydrocephalus secondary to cysticercal meningitis, and are associated with a high mortality rate (50%).21 Giant neurocysticercosis is defined as neurocysticercosises with a largest dimension of more than 4 or 5 cm.22 Racemose neurocysticercosises are rarely seen in India.23
MICROSCOPIC EXAMINATION
Racemose neurocysticercosis represents cysticercal decay with cyst enlargement and hydropic changes.24 Racemose cysticerci do not usually contain scolices and are considered nonviable encysted organisms. The degenerated vesicle wall is characteristically convoluted with external bulbous projections, and evokes an inflammatory response. The associated reactive process can also cause meningitis or arteritis.25
CLINICAL PRESENTATION
Meningeal, intraventricular, and subarachnoid (cisternal) forms
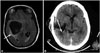
Racemose neurocysticercosis usually presents as a meningeal, intraventricular, or subarachnoid (cisternal) form (Figs. 2 and 3). The meningeal form presents with raised intracranial pressure due to various causes. It causes widespread meningitis and adhesions that result in cerebrospinal fluid (CSF) obstruction and hydrocephalus. It may subsequently cause vasculitis and entrapment of the cranial nerves in the inflammatory exudate, resulting in a focal neurological deficit.2627 Entrapment of oculomotor nerves may cause extraocular muscle paralysis and diplopia. The optic nerve and optic chiasm may become encased within the exudate, causing decreased vision and visual field defects.2829 In the intraventricular and subarachnoid (cisternal) forms, the oncospheres reach the ventricles via the choroid plexus. These parasites occlude the CSF pathway causing acute episodes of ventriculomegaly and a mass effect. Death of the larva causes ependymitis, which cause ventricular outlet obstruction and hydrocephalus.30 Patients present with raised intracranial pressure due to hydrocephalus secondary to basal meningitis and ependymitis.19 Ependymitis may cause ventricular entrapment, causing double-compartment syndrome.18
Neurocysticercosis, and in particular the subarachnoid forms, may produce cerebrovascular disease including cerebral infarction, transient ischemic attacks, and cerebral hemorrhage.3132 The most common underlying mechanism is the induction of arteritis.3334 Barinagarrementeria et al.35 found that 54% of 28 patients with subarachnoid forms of neurocysticercosis had angiographic evidence of cerebral arteritis. They reported that the middle cerebral and posterior cerebral arteries were the most commonly involved cerebral vessels associated with clinical stroke syndromes.35 Middle-sized cerebral blood vessel involvement is a common finding in subarachnoid forms of neurocysticercosis. Small- or large-vessel involvement may also cause infarcts in subarachnoid neurocysticercosises.36 Three cases of stroke secondary to neurocysticercosis were reported by Rocha et al.37: one patient had stroke secondary to subarachnoid cysts, causing bilateral middle cerebral artery occlusion that was angiographically proven; the second patient had arteritis of the basilar and carotid arterial systems secondary to cisternal cysts; and the third patient had vasculitis of the small cortical vessels.
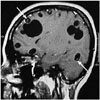
The intraventricular form of neurocysticercosis requires prompt, aggressive intervention in view of their rapidly progressive clinical course, and is often associated with a poor prognosis. It may occur along with the parenchymatous form or (more commonly) in isolation. The fourth ventricle is the most-common site (53%), followed by the third ventricle (27%), lateral ventricle (11%), and the aqueduct (9%).17 Mobile cysts within the lateral ventricle migrate toward the fourth ventricle due to the effects of gravity. They become entrapped in the fourth ventricle due to the size of the foramina of Magendie and Luschka. Patients with lateral ventricle cysticerci suffer from increased intracranial pressure with compression of the adjacent structures.3839 Patients with third-ventricular cysticerci present with sudden loss of consciousness due to acute hydrocephalus or progressively worsening headache and vomiting.1318 Cysts in the fourth ventricle present with subacute hydrocephalus with signs of brainstem dysfunction.40 Fourth ventricle cysts can also induce Bruns' syndrome, which is characterized by episodic headache, vomiting, papilledema, neck stiffness, and sudden positional vertigo induced by rotatory movements of the head, drop attacks, and loss of consciousness with rapid recovery. Rodriguez et al.41 reported a similar syndrome due to racemose neurocysticercosis involving the lateral, third, and fourth ventricles, basal cistern, and pineal region (Figs. 4 and 5). The exact pathomechanism of Bruns' syndrome remains unclear. The symptoms may occur due to episodic elevation of intracranial pressure as a result of changes in the cyst position, with a change in head posture causing blocking of the ventricular outflow via a ball-valve mechanism.4243
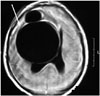
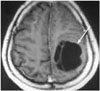
In rare cases racemose neurocysticercosis can cause dementia as a sole presenting feature in the patient.44 However, 66-87.5% of patients with neurocysticercosis have been reported to have cognitive disturbances, and dementia or severe cognitive decline has been reported in 12.5-15.6% of patients.454647 The mechanisms proposed for cognitive decline in neurocysticercosis include raised intracranial pressure, number and location of neurocysticercosises, different phases of evolution, inflammatory cytokines, and the host's immune response.45 The reversibility of dementia depends upon the predominant underlying mechanism. Dementia due to raised intracranial pressure as an underlying mechanism has an excellent outcome as compared to multiple parenchymal parasitic and vascular lesions. Racemose neurocysticercosis can also present with a mass effect (Figs. 6 and 7).48 There are reports of racemose neurocysticercosis occurring in the cerebellar hemisphere.49
Spinal form
Involvement of the spinal cord in neurocysticercosis is rare, reportedly accounting for 1-5% of all cases of neurocysticercosis.50 Spinal neurocysticercosis can present as leptomeningeal (extramedullary) or intramedullary forms, with the former being six to eight times more common than the latter. They are the extension of a cerebral subarachnoid disease to the spinal subarachnoid space. Cysts may be singular or may form into clumps of several cysts distributed throughout the spinal subarachnoid space.5152 The intramedullary form occurs commonly in the thoracic spinal cord and is secondary to hematogenous or ventriculoependymal migration.5354 Spinal leptomeningeal neurocysticercosis is difficult to treat, especially if it is associated with arachnoiditis, and has a poor prognosis.55 The clinical manifestations of racemose neurocysticercosis are listed in Table 1.
RADIOLOGICAL INVESTIGATIONS
Computed tomography of the head
Computed tomography (CT) of the head has a sensitivity and specificity of more than 95% in the diagnosis of the parenchymatous form of neurocysticercosis.5657 However, it has lower sensitivity and specificity for diagnosing the ventricular and cisternal forms. These scans are helpful in detecting calcifications. Parenchymal forms of neurocysticercosis appear as single or multiple rounded lesions of low density with an eccentric mural nodule representing the scolex. The administration of contrast agent results in ring enhancement of the wall of the cyst, reflecting an inflammatory reaction. The intraventricular cysts produce dilatation of the ventricles depending on their location. Ventricular or periventricular enhancement suggests ependymitis. The presence of a ventricular cyst can be distinguished from inflammatory ventricular obstruction by positive contrast ventriculography. The presence of a regular, rounded filling defect similar to an inverted cup suggests the presence of a cyst, whereas a cul-de-sac suggests inflammatory ventricular obstruction.58 Intraventricular cysts are difficult to detect via brain CT. They appear isodense with the CSF and have thin walls, and therefore are not well visualized.
MRI of the brain
The cisternal or ventricular forms of neurocysticercosis are easily missed in CT scans, but are readily visualized in MRI. The subarachnoid cysts over the convexity of the cerebral hemispheres are small, but those in the Sylvian fissure may reach 50 mm or more in size. MRI is suitable for the identification of small parenchymal cysts-those located in the base of the brain, ventricles, and spine.10 It allows assessment of the degree of infection, the location, and the stage of the cyst in the brain.59 MRI is helpful for identifying leptomeningeal enhancement at the base of the brain secondary to arachnoiditis in cases of subarachnoid cysts.10 Intraventricular cysts have attenuation and signal intensity values similar to the CSF, and the cystic wall is very thin.6061 Conventional MR sequences such as T1- and T2-weighted images and fluid-attenuated inversion recovery images may miss intraventricular/cisternal neurocysticercosis cysts.62 The optimal MR protocol for identification of intraventricular cysts and scolex is controversial. Three-dimensional (3D), very heavily T2-weighted sequences, such as constructive interference in steady state or fast imaging employing steady-state acquisition, are good sequences for evaluating intraventricular cysts.62 These MR sequences have a high spatial resolution and signal-to-noise ratio. Another MR sequence that is also useful is the 3D spoiled gradient recalled echo sequence,63 which provides T1 information. Intraventricular cysts may also move within the ventricular cavities in relation to head movement (ventricular migration sign).64
SEROLOGY
Serological tests should detect antibodies specific for T. solium antigens for the clinical diagnosis of neurocysticercosis. The current test of choice is electroimmunotransfer blotting, which has a sensitivity of 94-98% and a specificity of 100% for patients with two or more cysts or enhanced lesions.6566 However, the sensitivity is lower in patients with solitary enhanced or calcified lesions.67 Another test is the enzyme-linked immunosorbent assay (ELISA), which is neither sensitive nor specific.68 Along with antibody assays, circulating parasite antigen assays are available that reflect the presence of live parasite and may aid in quantitative verification of successful treatment.697071 Ag-ELISA based on the monoclonal antibody reacting with a repetitive carbohydrate epitope of secretory/excretory and surface antigens of live cysticerci has been applied.72 This assay has a sensitivity of 86% and a specificity of 96%,73 and has been used for evaluating the treatment response for subarachnoid cysts in a small number of patients.74 This antigen assay should be used to follow up patients with subarachnoid cysts. Serological tests should be used in conjunction with clinical and radiological data.75
TREATMENTS
The treatment modalities available in patients with neurocysticercosis include medical management with cysticidal agents, corticosteroids, and antiepileptic drugs, and surgical management to remove the cyst or to insert a shunt to treat hydrocephalus.
Cysticidal agents
There has been controversy as to whether cysticidal drugs modify the natural history of neurocysticercosis. There are arguments against the use of cysticidal drugs: 1) the cysts usually die within a short time interval and treatment may be unnecessary,76 2) scarring due to increased inflammation following initiation of drugs may worsen the long-term prognosis of seizures,77 and 3) increased inflammation due to death of the cysts. According to Salinas and Prasad.78 there is insufficient evidence to assess the beneficial effects of cysticidal drugs in neurocysticercosis.
Praziquantel and albendazole are cysticidal drugs that are effective in the treatment of all forms of neurocysticercosis.7980 Praziquantel is an isoquinolone that causes spastic paralysis of the parasite, while albendazole is an imidazole that acts by inhibiting glucose uptake by the parasites, causing energy depletion. There are no available controlled trials on the management of subarachnoid cysts. Cysticidal drugs are applied for longer when treating giant cysts and subarachnoid cysts than when treating parenchymal neurocysticercosises.2 The disappearance of intraventricular and subarachnoid cysts with cysticidal drug therapy has been reported.81 The administration of albendazole at a higher dose (30 mg/kg/day) than usual has been found to increase the clearance of intraventricular and subarachnoid cysts.82 In the treatment of intraventricular and subarachnoid cysts, a ventriculoperitoneal shunt must be placed in patients with significant obstructive hydrocephalus.83 Steroids should be given before initiating cysticidal drugs in patients with intraventricular and subarachnoid cysts in order to reduce the inflammation and the risk of shunt obstruction.84 Oral prednisolone should be given 2-3 days before initiating cysticidal drugs and continued for at least 7-10 days. In a study of 33 patients with giant subarachnoid cysts treated with albendazole (15 mg/kg/day for 4 weeks), Proaño et al.83 found that several courses of therapy were required for effective treatment. Methotrexate has been used as a steroid-sparing agent in patients with subarachnoid disease requiring long-term steroids.85
Surgical management
Cisternal forms
Racemose cysts in the basal cisterns of the brain cause symptoms secondary to local compression. They are usually associated with local adhesions secondary to inflammation. Excision of cysts is not recommended due to the possible presence of severe adhesions.
Intraventricular/subarachnoid forms
The surgical indications for excision are a mass effect, obstructive hydrocephalus, fourth ventricular cyst, and uncertain diagnosis. The surgical resection of ventricular cysts is by microsurgery and/or endoscopy. Acute hydrocephalus due to ventricular cysts mandates an emergency ventriculostomy to relieve the raised intracranial pressure, followed by cyst resection. A ventriculoperitoneal shunt must be placed if there is associated ependymitis. Shunt failure rates are reportedly as high as 30-70%. As a result, patients may require multiple shunt revisions, which are associated with a high mortality rate.408687 Microsurgical excision of fourth-ventricular cysts via a posterior fossa craniotomy, and supratentorial open or stereotactic craniotomy for lateral- or third-ventricular cyst excision have been described.88 However, endoscopic approaches have more recently become the treatment of choice.899091929394 The advantages of the neuroendoscopic approach include easy navigation within the ventricles and the ability to excise multiple cysts with minimal postoperative complications.9596 However, the potential limitations of the neuroendoscopic approach include intraventricular bleeding, and this procedure may be hazardous in the presence of ependymitis and dense adhesions.97 Patients with intraventricular cysts with significant ependymal enhancement are thus poor candidates for the neuroendoscopic approach. It has been reported that aspiration of the cyst contents prior to its removal in order to collapse it makes the cyst easier to handle and excise.98
CONCLUSION
Neurocysticercosis is the most common parasitic disease of the CNS and is caused by the metacestode larva of the pork tapeworm, T. solium. In the CNS, the cysticerci can present as either a parenchymal form (cysticercus cellulosae) and/or an extraparenchymal form, as racemose cysts in the subarachnoid spaces, basal cisterns, and within the ventricles. Racemose cysts are a less frequent presentation of neurocysticercosis. The presentation and management of the two forms is different. They present with raised intracranial pressure secondary to hydrocephalus, mass effect, meningitis, and vasculitis. Other manifestations include Bruns' syndrome and dementia. The investigation of choice for the diagnosis of racemose cysts is MRI. Due to its multiform manifestation, less frequent occurrence, and chances of false negativity on imaging, a high index of suspicion for the diagnosis is mandated, especially in endemic areas.
SEARCH STRATEGY AND SELECTION CRITERIA
References for this review were identified by searches of the PubMed database from 1952 to September 2013, using the terms "Racemose neurocysticercosis," "neurocysticercosis," and "intraventricular cysticercus." Additional references (including abstracts) and book chapters cited in relevant articles were also reviewed. Most papers used in this review were published in English, although non-English articles with English abstracts were included when relevant.




 XML Download
XML Download