

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The effect of granulocyte colony-stimulating factor (G-CSF) on the course of neurological diseases has drawn considerable attention over the past decade. G-CSF mobilizes hematopoietic (CD34+) stem cells and-with repeated administration-recruits immature CD34+/CD133+ stem cells that are capable of differentiating into neuronal progenitors.1,2 G-CSF receptor expression may play an autocrine protective role in various cells of the nervous system,3 and G-CSF may protect against ischemic neuronal damage by inhibiting apoptosis and inflammation, mobilizing stem cells, or enhancing neuronal differentiation.3,4
Recent studies have suggested a role for G-CSF in the treatment of amyotrophic lateral sclerosis (ALS).5,6,7,8,9 In a mouse model of ALS, G-CSF significantly improved motor performance and motoneuron survival, and reduced denervation atrophy.10 A study involving subjects with ALS found significantly reduced G-CSF receptor expression in motoneurons and increased G-CSF expression in reactive astrocytes.8 The authors suggested that reduced G-CSF receptor expression on motor neurons might account for the pathophysiology of ALS. Simultaneously the levels of monocyte chemoattractant protein-1 (MCP-1) were increased, suggesting that reduced-CSF receptors can exacerbate the ALS course.
Most studies of G-CSF efficacy in subjects with ALS have been limited in several ways. A nonrandomized study involving 13 subjects with ALS demonstrated a significantly lower monthly reduction in ALS Functional Rating Scale-Revised (ALSFRS-R) scores and compound motor action potential (CMAP) amplitude following 5 days of G-CSF treatment.9 Another uncontrolled study involving 24 individuals did not show any significant effect of G-CSF on clinical outcomes.11 In a placebo-controlled study of G-CSF treatment in ten subjects with ALS, G-CSF treatment failed to improve any of the clinical outcomes, although it significantly reduced the fractional anisotropy on diffusion tensor imaging.12 Finally, a double-blind study involving 39 subjects found no statistically significant benefit with G-CSF, although there was a trend toward slowing of disease progression following two cycles of G-CSF treatment.13 One problem with that study was that more than 50% of the subjects were lost to 1-year follow-up.
The present study was a randomized double-blind, placebo-controlled trial of G-CSF with assessment of various clinical, functional, electrophysiological, and molecular outcomes, the aim of which was to provide a thorough view of the efficacy of G-CSF and its tolerability in Iranian subjects with ALS, and to address some of the caveats noted in previous studies.
METHODS
Trial design and setting
This was a single-center, 3-month, randomized, double-blind, placebo-controlled, and parallel-group study that was conducted in a tertiary referral center affiliated with Tehran University of Medical Sciences between November 2012 and November 2013.
Participants
Male and female subjects with a diagnosis of probable or definite ALS based on the revised El Escorial World Federation of Neurology criteria were screened for inclusion in the study. The following inclusion criteria were applied: aged 18-85 years, symptom history not exceeding 2 years, and ALSFRS-R score ≥20. Although ethnicity was not an inclusion criterion, all of the subjects were ethnically Iranian. Riluzole treatment was not an exclusion criterion if the patient had been stable on the therapeutic protocol for at least 30 days prior to study entry. The following exclusion criteria were applied: ALS in first-degree relatives; pregnancy or lactation; history of neoplasia, myeloproliferative, or any other disorders that could be exacerbated by G-CSF; active immunological disease; spleen diameter ≥180 mm; severe heart, kidney, or liver disease, positive HIV status, forced vital capacity ≤50% of that predicted; cognitive disorders that interfere with the study procedure; and history of hypersensitivity reaction to GCSF or Escherichia-coli-derived proteins.
After receiving a complete explanation of the study procedures, all subjects (or their representatives) provided written informed consent to participate prior to study entry. The study protocol was approved by the Ethics Committee and the Institutional Review Board of Tehran University of Medical Sciences (approval no. 91-01-54-17265). The trial was conducted in accordance with the last revision of the Declaration of Helsinki and was registered at ClinicalTrials.gov (registration no. NCT01825551).
Study procedures
The subjects underwent a complete physical and neurologic examination, peripheral blood smear, complete blood count with differentials, liver enzymes, serum lactate dehydrogenase (LDH), uric acid, CD34+ and CD133+ cell count, serum and cerebrospinal fluid (CSF; in a subset of subjects) MCP-1 levels, abdominal ultrasound (if the spleen was palpable), and pulmonary function testing (if significant respiratory dysfunction was present). Scores for the ALS Assessment Questionnaire-40 (ALSAQ-40), ALSFRS-R, and manual muscle testing (MMT) were assessed every month. Nerve conduction velocity (NCV) studies were performed by an expert (A.T.) at baseline and at the study endpoint. The white blood cell (WBC) count was measured every day during the treatment phase. WBC differentials, liver enzymes, and CD34+ and CD133+ cell counts were measured on days 4 and 6, and LDH and uric acid levels were assessed on day 4 of the trial. MCP-1 concentration was only tested at baseline.
Subjects were randomly assigned to receive either subcutaneous G-CSF (containing PDgrastim, filgrastim, 300-µg recombinant G-CSF, equal to 30,000,000 IU of filgrastim, mannitol, and sodium acetate; Pooyesh Darou, Tehran, Iran) 5 µg/kg/q12h or normal saline for five consecutive days. The subjects were hospitalized and closely monitored for any possible serious adverse events during the first few days. Treatment was discontinued if the leukocyte count rose to more than 50,000/µL; the remaining doses were administered when levels had returned to lower values (below 15,000/µL). The participants were then followed up in the outpatient clinic.
Assessments
Amyotrophic lateral sclerosis Functional Rating Scale-Revised is a 12-item (total score of 0-48) physician-administered measure of ALS severity that assesses function in three major domains: bulbar, motor, and respiratory. Each item is scored on a five-point scale (0-4), with higher scores reflecting better function.14
Amyotrophic lateral sclerosis Assessment Questionnaire-40 is a 40-item subjective measure of health status for subjects with ALS that is categorized into five domains: eating/drinking, communication, activities of daily living/independent activities of daily living, physical mobility, and emotional functioning. The total ALSAQ-40 score and those of its domains are converted into a 100-point scale, with lower scores reflecting a better health status.15,16
Manual muscle testing was based on the examination of 34 muscles, converted to a 10-point scale. The final MMT score is the mean of the scores for all 34 muscles. MMT appears to be the preferred method for measurement of global strength.17
The NCV studies involved a belly-tendon montage of CMAP amplitude recordings from the median (abductor pollicis brevis), ulnar (abductor digiti minimi), tibial (abductor hallucis brevis), and common peroneal nerves (extensor digitorum brevis). CMAPs were recorded in response to supramaximal stimulation with 0.2-ms duration.
Outcome measures
The primary outcome measure was the monthly rate of decline in ALSFRS-R score. Secondary outcome measures were the changes from baseline in the ALSAQ-40 and MMT scores, and the CMAP amplitude of the nerves. Furthermore, the correlations between MCP-1 levels, counts of CD34+, CD133+, and CD34+/133+ cells, and ALSFRS-R scores were calculated. Safety issues were systematically assessed using both a checklist for clinical symptoms and laboratory values.
Randomization, allocation concealment, and blinding
A randomization list was prepared using a computerized random-number generator in a 1:1 ratio and block size of four. Allocation concealment was achieved using sequentially numbered and opaque envelopes. Treatment allocation, evaluation of side effects, and possible changes in treatment protocol, clinical rating, and electrophysiological assessment of the subjects were conducted by separate researchers. The subjects, the evaluator, the person responsible for administering the intervention, and the statistician were all blind to the treatment allocation.
Statistical analysis
STATA version 12.0 (StataCorp, College Station, TX, USA) was used for the data analysis. All analyses were carried out on the data from participants with at least one postbaseline measurement. Per-protocol and linear mixed model analyses were both used for comparison of outcomes. Repeated-measures linear mixed model analysis was performed using the STATA module for analyzing repeated-measures data (xtmixed), which can account for unbalanced data. Except where stated otherwise, the data are presented as mean±SD values, and the cutoff for statistical significance was set at p<0.05.
The sample size was calculated based on a between-group difference of three (with a standard deviation of three) for the change in ALSFRS-R scores from baseline. This yielded a sample size of 16 in each group, and accounting for a potential 20% loss to follow-up, a sample size of 40 was reached.
RESULTS
Baseline characteristics and laboratory values
Sixty-seven subjects were screened for eligibility criteria and 40 subjects were randomized into either the G-CSF (n=20) or placebo (n=20) group. All subjects had at least one postbaseline measurement, and 35 subjects completed the study (n=18 and 17 for the G-CSF and placebo groups, respectively). The baseline characteristics of the subjects are summarized in Table 1. One patient experienced transient fever and chills at day 4 of treatment.
The WBC count in the G-CSF group rose from 7,892±2,009/µL at baseline to 49,689±14,613/µL at day 6 (p<0.001, repeated-measures ANOVA), whereas no significant change was observed in the placebo group (7,041±1,613/µL and 6,862±1,312/µL at baseline and day 6, respectively; p=0.985). The numbers of neutrophils, CD34+, CD133+, and CD34/133+ cells increased significantly in the G-CSF group (p<0.01 for all), but not the placebo group. Of the laboratory tests, alkaline phosphatase and LDH levels increased significantly in the G-CSF group.
ALSFRS-R scores
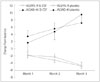
Both groups exhibited a progressive decline in the ALSFRS-R score (p<0.0001 for time effect). In the mixed model analysis, no significant time-treatment interaction was observed (Fig. 1, Table 2). The per-protocol analysis (Table 3) revealed that the monthly reduction in ALSFRS-R scores did not differ significantly between the G-CSF group (1.53 points/month) and the placebo group [1.61 points/month; mean difference (95% CI)=0.074 (-0.952 to 1.101), t (34)=0.146, p=0.884].
NCV
Except for one of the measurements (right common peroneal), changes from baseline did not differ significantly between the two groups (Table 4).
Association between CD34+ (CD133+) cell count, MCP-1 level, and ALSFRS-R score
In the G-CSF group, changes in the CD34+ cell count in the first 6 days were negatively correlated with the ALSFRS-R score reduction (r=-0.485, p=0.041). Further analysis revealed that those with large changes in CD34+ (>100/µL) cell count did not differ significantly from the placebo group in terms of reduction in ALSFRS-R scores. The elevation in the CD34+ cell count was lower in the females than the males of the GCSF group, with the difference tending toward significance (55.9±45.7/µL vs. 106.2±61.8/µL; p=0.062, Mann-Whitney U-test). Further exploratory analysis demonstrated that female subjects in the G-CSF group tended toward a greater reduction in ALSFRS-R scores than their counterparts in the placebo group (p=0.073). Changes in CD133+ (r=-0.102, p=0.687) or CD133+/CD34+ (r=-0.323, p=0.190) cell counts were not significantly associated with ALSFRS-R reduction.
Baseline CSF MCP-1 levels were positively correlated with the change in ALSFRS-R scores in both groups (Spearman's ρ=0.370, p=0.070). No significant correlation was observed between the serum levels of MCP-1 and ALSFRS-R scores.
DISCUSSION
In the present study, although G-CSF treatment increased the WBC (and CD34+/CD133+ cells) count to the expected range, it failed to improve any of the study outcomes in the subjects. Furthermore, an elevation in the CD34+ and CD133+ counts was not correlated with better outcomes. These findings, together with most previous studies demonstrating little clinical advantage with G-CSF use in subjects with ALS, suggest that G-CSF administration with current protocols is unlikely to be of any clinical benefit in subjects with ALS.
An important question is thus raised as to why, despite promising preliminary data, G-CSF failed to improve clinical outcomes in subjects with ALS. G-CSF can pass through the blood-brain barrier (BBB) in rats, but human data are not yet available.13,19 However, the neuroradiological changes observed following G-CSF administration in humans could be taken as evidence of the ability of this growth factor to exert its effects beyond the BBB.12 Furthermore, the findings of a separate line of studies suggest that G-CSF has direct neuroprotective properties through immunomodulation or counteraction of apoptotic pathways.5,10 Another reason for the lack of a G-CSF effect might be inadequacy of the duration or dose of treatment.12 All clinical studies to date have used one or only a few cycles of G-CSF with up to 1 year of follow-up, and found only minor differences in clinical outcomes. Therefore, within the range of currently routine protocols, it is unlikely that extended follow-up periods will yield additional clinical benefits of G-CSF administration. Conversely, studies of G-CSF administration in a mouse model of ALS employed much higher doses (up to 100 µg/kg body weight), which may account for the observed difference in the outcomes between human and animal studies.7,10
In the present study, the elevation in CD34+ cell count was positively correlated with a better clinical response. In further exploratory analysis it was determined that the lower CD34+ count and lower clinical response in the females of the G-CSF group accounted for this finding. G-CSF did not improve the ALSFRS-R score in the females; indeed, it appeared to aggravate it compared to placebo. The lower CD34+ cell count observed in the females is probably an innocent-bystander phenomenon, because healthy females generally have a lower CD34+ cell yield following G-CSF treatment.20 Furthermore, the greater symptom progression in the females of the G-CSF group is unlikely to be related to the predictive role of female gender in disease progression, because similar findings were not observed in the females of the placebo group.21 Together these exploratory findings raise the possibility that G-CSF exacerbates the course of ALS in female subjects. However, our study was not designed to analyze outcomes based on gender subgroups, and therefore further investigation is required to address this finding.
The present study demonstrated a trend toward a faster symptom progression in subjects with higher baseline CSF MCP-1 concentrations. As a multifunctional chemokine, MCP-1 is involved in several inflammatory, allergic, and immunodeficiency conditions.22 Importantly, MCP-1 can increase BBB permeability to monocytes and dendritic cells, and can thus exacerbate inflammation.23 Accordingly, elevated MCP-1 serum and CSF concentrations may hasten neuronal death by enhancing inflammation in ALS.8,23
This study was limited by its short duration. However, findings of previous studies suggest that a longer duration of follow-up is unlikely to confer any important clinical benefit with currently administered doses of G-CSF. We recruited a relatively large number of subjects compared to other published trials of G-CSF in subjects with ALS. However, there were still near-significant p values in some of the secondary outcomes, and it is possible that type II errors were present due to the smallness of the sample.
While this study is not entirely novel, it has some distinctive features. Given that ALS exhibits a diverse risk profile across ethnicities,24 genetic background and therefore response to treatment might also differ across populations. Thus, this study can be considered an account of how Iranian ALS subjects respond to G-CSF. This might also be the reason for some of the subtle differences between the findings of this study and others. This study had several strengths. The stringent eligibility criteria led to the recruitment of a homogeneous patient population. Data from all subjects were entered into intention-to-treat analysis, and the final dropout rate was only 10%. Although the short study duration is probably one reason for the low number of dropouts, at the same time the short-spaced follow-ups provide a clearer view of the disease response in the short term. Moreover, the assessment of several aspects (e.g., clinical and functional) of ALS in our subjects ensures that the lack of G-CSF efficacy is not due to insensitivity of some of the measurement instruments.
In summary, although short-term G-CSF treatment was found to be safe in this study, there was little evidence of its efficacy in subjects with ALS. If G-CSF is to be tested further in studies of subjects with ALS, it probably should be administered with a different dose or delivery protocol (e.g., high dose or intraspinal delivery) and with greater caution in females.


 XML Download
XML Download