

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Carotid artery stenosis (CS) is one of the most significant risk factors for ischemic stroke.1 Chronic cortical hypoperfusion arising from CS is currently being investigated as an important source of cognitive impairments, regardless of whether it accompanies stroke.2 The artery-to-artery embolism caused by CS can result in multiple infarcts, leading to vascular cognitive impairments and vascular dementia. Furthermore, in cases of severe CS, perfusion defects can arise in the affected areas of the cerebral cortex, which may result in cognitive impairments associated with those defects.3,4,5,6 Therefore, when carotid artery stenting (CAS) procedures are undertaken to widen a narrowed area, it is predicted that the improved perfusion in the stenosed area of the cortex will lead to a recovery of cognitive functions and eventually help to reduce the risk of vascular cognitive impairments and vascular dementia.7,8 However, it has also been reported that cognitive function can be negatively affected due to microembolisms caused during the CAS procedure itself, or temporary perfusion defects that may take place during balloon dilatation. Thus, studies are needed to determine whether CAS has any impact on the cognitive function of patients with CS; such studies should involve detailed neuropsychological tests before and after the CAS procedure. Little research has been done in this area to date.9,10
The present study compared the cognitive performance of patients with symptomatic CS and asymptomatic severe CS (≥70%) by testing their cognitive function prior to CAS and 3 months thereafter. Their neuropsychological test results were also compared with those of a control group consisting of CS patients who had not received the CAS procedure, in order to assess whether there are any meaningful differences between the two groups.
METHODS
This prospective, single-center study was conducted at Dong-A University Hospital for 3 months from February 2009 until December 2012. The study was approved by the Institutional Review Board of Dong-A University Hospital with respect to the clinical protocol, informed consent form (ICF), and patient information sheet (PIS). All subjects voluntarily consented to participate in the study by submitting their ICF after being provided with all relevant information related to the study through the PIS, including their right to freely withdraw from the study at any point.
Subjects
This study involved both symptomatic and asymptomatic CS patients who visited the Department of Neurology or the Stroke Center of Dong-A University Hospital as outpatients or emergency patients. The symptomatic CS patients had within the previous 6 months experienced at least one transient or mild symptomatic ischemic vascular event in the distribution of one or both internal carotid arteries. Patients who met any of the following criteria were excluded from the study: 1) severe language disorders or motor weaknesses caused by acute cerebral infarction; 2) acute confused state lasting for at least several days; 3) brain tumor, infection, or other diseases as diagnosed by brain imaging; or 4) a history of depression, head injury, drug abuse, or similar trauma that could impact their cognitive functioning. The control group consisted of patients who had been diagnosed with CS by diagnostic neuroangiography, but who did not undergo CAS.
Neuropsychological screening
The subjects' overall cognitive performance was evaluated using the Korean version of the Mini Mental State Examination (K-MMSE),11,12 and more detailed tests were performed based on the Seoul Neuropsychological Screening Battery-Dementia Version (SNSB-D).13 The neuropsychological tests were performed within 14 days after the onset of stroke symptoms or signs. The SNSB-D comprises five test subcategories with a total possible score of 300: attention, 6% (17 points); language function, 9% (27 points); visuospatial function, 12% (36 points); memory function, 50% (150 points); and frontal lobe executive function, 23% (70 points). Attention was evaluated using the digit span test-forward and digit span test-backward, and visuospatial function was assessed using the Rey-Osterrieth Complex Figure Test (ROCFT). Memory was tested by evaluating both verbal memory and nonverbal memory. Verbal memory was assessed based on the capacity for immediate recall, delayed recall, and the recognition domain of the Seoul Verbal Learning Test (SVLT). Nonverbal memory was measured based on the capacity for immediate recall, delayed recall, and the recognition domain of the ROCFT (ROCFT-recognition). Frontal executive function was evaluated by conducting contrasting-program, go-no-go, fist-edge-palm, word fluency-animal, word fluency-phonemic, and Stroop tests. Finally, language and related functions were assessed using the Korean version of the Boston Naming Test,14 and calculation and apraxia tests.
Carotid ultrasonography brain imaging, and operative procedures
Brain magnetic resonance imaging (MRI)/magnetic resonance angiography imaging (1.5-tesla GE MRI scanner, GE Healthcare, Piscataway, NJ, USA) was performed on all patients, as were carotid ultrasonography and neuroangiography. The existence and severity of a CS in the participating patients were evaluated by a single neuroradiologist who conducted neuroangiography based on the North American Symptomatic Carotid Endarterectomy Trial.15 Measurements of the site, severity, and length of the stenosis, the plaque characteristics, and the vessel were performed in order to select an appropriately sized the balloon and stent in cases submitting to the CAS intervention. CAS was performed in a dedicated operating room equipped for endovascular procedures, under local anesthesia, and through a femoral approach. Cerebral protection devices were used to prevent microembolisms during the procedure.
Statistical analysis
Statistical analyses were performed using SPSS version 22 (SPSS Inc., Chicago, IL, USA), and in principle the two-tailed test was performed when p≤0.05. The demographic data and neuropsychological test results of the subjects were reviewed using SPSS descriptive statistical analysis. With respect to the subjects' demographic data and baseline scores, the average values were compared between those patients who underwent CAS (the stent treatment group) and the unstented control group using the independent-samples t-test. For categorical variables, frequencies were compared using the chi-square test.
Since the neuropsychological tests were conducted for both the stent treatment group and the control group, baseline scores and scores achieved at the 3-month follow-up were compared within each group for the respective cognitive test categories. In the analysis, the covariates included subject age, for which meaningful differences were found between the stent treatment group and the control group, and baseline scores. Analysis of covariance (ANCOVA) was conducted to analyze changes in the neuropsychological test scores between baseline and the 3-month follow-up. Furthermore, by applying the same method, symptomatic and asymptomatic CS patients were separately compared with the control group to determine the effects of reperfusion following the CAS procedure. In addition, patients in the stent treatment group were assigned to the following subgroups according to the presence of factors that were expected to affect cognitive function: 1) patients with microembolism based on brain diffusion-weighted MRI performed after the CAS procedure, 2) patients with perfusion defects based on brain perfusion MRI, and 3) patients with CS (≥70%) in the left carotid artery. The neuropsychological test score changes between baseline and the 3-month follow-up of these three subsets of patients were each compared with those of the control group.
Except where stated otherwise, the data are presented as mean±SD values.
RESULTS
Twenty-three of the 31 patients in the stent treatment group and 10 of the 11 patients in the control group completed the 3-month follow-up tests. The reasons for loss to follow-up in the stent treatment group were withdrawal of informed consent (n=6) and no 3-month follow-up test (n=2), while one patient in the control group did not receive the 3-month follow-up test. These nine patients were treated as losses to follow-up and were excluded from the analyses; thus data from 23 patients in the stent treatment group and 10 control subjects were analyzed.
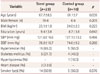
The demographic data and medical characteristics of the stent treatment and control subjects are listed in Table 1. The age differed significantly (p=0.039) between the stent treatment group (67.7±8.5 years) and the control group (61.1±7.0 years), but none of the other characteristics differed significantly between the two groups. Therefore, all of the analyses were conducted after adjusting for age based on ANCOVA. The stent treatment group comprised 19 males (82.6%) and had an average of 9.4 years of education; the corresponding values for the control group were 6 males (60.0%) and 8.7 years. The most common vascular risk factor was high blood pressure in both the stent treatment group and the control group (frequencies of 65.2% and 50.0%, respectively), followed by smoking, diabetes, heart diseases, and hyperlipidemia. The stent treatment group contained 11 symptomatic CS patients and 12 asymptomatic CS patients. Nine of these 23 patients submitted to MRI (including diffusion-weighted MRI), which revealed that 5 patients had developed a microembolism due to the CAS procedure. Five of the 19 patients for whom brain perfusion MRI was performed were found to have perfusion defects at a meaningful level. Finally, the CS was on the right side in 14 patients, on the left side in 8, and bilateral in 1 (Table 2).
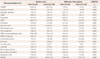
The changes in cognitive performance of the patients in the stent treatment and control groups between baseline and the 3-month follow-up are given in Table 3. The stent treatment group had average baseline K-MMSE and SNSB-D scores of 25.0 and 152.5 points, respectively; these scores had increased by 1.3 and 17.6 points, respectively, at the 3-month follow-up. However, the scores in the control group had also increased, by 1.1 and 17.3 points, respectively, in the follow-up test compared to baseline. These findings indicated that there was no statistically significant improvement in test scores between the patients and control group. From a clinical point of view, the participating patients exhibited improvements in all test categories of neuropsychological assessment except for the drawing of a Luria loop. However, the level of improvement in the stent treatment group was not statistically meaningful when compared with the control group. In fact, in the test of SVLT-recognition, the control group achieved a more statistically meaningful improvement than the stent treatment group.
Symptomatic CS patients had average K-MMSE and SNSB-D scores of 23.5 and 142.5 points, respectively; the corresponding values for the asymptomatic CS patients were 26.3 and 161.7 points. At the 3-month follow-up test the K-MMSE scores of the two groups were 1.8 and 0.3 points higher, respectively, than their baseline scores, and their total SNSB-D scores had increased by 32.3 and 4.2 points. When compared to both the asymptomatic CS patients in the stent treatment group and the control group, symptomatic CS patients exhibited statistically meaningful improvements in ROCFT, ROCFT-recognition, and total SNSB-D scores (Table 4). Conversely, asymptomatic CS patients exhibited declines in several test results, including the ROCFT, orientation, and phonemic and animal word fluency.
Additional analyses were conducted on subsets of patients possessing factors that were deemed to affect the cognitive function of patients with CS. Five (56.0%) of the nine patients for whom brain diffusion-weighted MRI was repeated after the CAS procedure were found to have a microembolism. Nevertheless, these five patients performed similarly on cognitive tests to patients without a microembolism (Supplementary Table 1 in the online-only Data Supplement). In order to determine whether the recovery from perfusion defects induced by a CAS procedure affects the cognitive functioning of patients with CS, cognitive performance was compared between patients with and without perfusion defects, as determined by brain perfusion MRI. Patients with perfusion defects that were improved by CAS achieved improved calculation test scores, which were on average 2.8 points higher than at baseline; this was a significant improvement compared with the control group (p=0.048). However, the group of patients who did not develop perfusion defects exhibited improvements in the immediate recall and recognition domains of the SVLT (p<0.05) (Supplementary Table 2 in the online-only Data Supplement). The location (left or right hemisphere) of the perfusion defect had no effect on cognitive performance changes (Supplementary Table 3 in the online-only Data Supplement).
DISCUSSION
The changes in cognitive performance of symptomatic and asymptomatic CS patients were analyzed in this study in a prospective manner by testing their cognitive function before and after the CAS procedure. The reliability of this study was enhanced by the additional comparison of the cognitive performance test results of these CS patients those of a control (non-CAS) group. The number of people suffering from arteriosclerosis with vascular risk factors has been increasing recently due to the westernization of diet patterns and changing living environments, which has led to increases in the number of patients with CS or cerebral infarction.15 Severe CS is one of the important culprits underlying cerebral infarction, and can cause cognitive impairments due to continuous perfusion defects.9,16
Until recently, many reports have focused on the effects of the revascularization procedure on the cognitive function of patients with CS. However, when it comes to the effects of carotid endarterectomy or CAS, the findings have been conflicting, with some researchers reporting improved cognitive performance7,8,17,18 and others reporting the opposite.19,20 Enhanced cognitive performance can result from the perfusion improvement due to revascularization as well as the subsequent recovery of cerebral cortex functioning. Meanwhile, any decline in cognitive performance likely stems from stenting-induced microembolism9,10,21 or temporary perfusion defects due to the balloon dilatation of a narrowed area.21
Examination of the demographic and social characteristics of the subjects in the present study revealed that high blood pressure was the most common vascular risk factor, followed by diabetes and heart diseases. These findings are in line with those of other studies.22
The stent treatment group exhibited clinical improvements over baseline in most of the test categories of the neuropsychological screening that was performed 3 months after the CAS. However, the improvement was not statistically meaningful since the control patients, who did not receive the CAS procedure also recorded improvements. Most previous research that demonstrated positive effects of CAS on cognitive function only compared the cognitive performance of patients before and after CAS, without comparing the cognitive performance improvement between the stent treatment group and a control group.9 The improvements in cognitive performance exhibited by the control group is likely attributable to learning effects, given that the follow-up cognitive testing was performed only 3 months after the baseline testing. A more accurate analysis and higher reliability require long-term tracking observations.23
Compared to the asymptomatic CS patients and the control group, the symptomatic CS patients recorded statistically meaningful improvements in cognitive function after the CAS procedure in terms of their total scores for ROCFT-recognition and SNSB-D. Therefore, CAS exerts meaningful effects on the cognitive function of symptomatic CS patients, which implies that asymptomatic CS patients suffer less in terms of cognitive impairment than do symptomatic patients.24 We cannot definitively explain the relatively greater improvement in visuospatial function compared with other cognitive domains observed in the present study. Pre- and post-CAS functional neuroimaging studies (i.e., brain single-photon-emission computerized tomography or positron-emission tomography) are needed to explore the appropriate area of functional improvement explained by cognitive domains after CAS.
The asymptomatic CS patients had a poorer cognitive performance after the CAS in the test categories for evaluating frontal executive function, orientation, the ROCFT, ROCFT-recognition, Luria loop, Stroop test, and word fluency, which was presumably due to microembolisms caused by the CAS. Nevertheless, patients who developed microembolism performed similarly on the neurophysiological test battery to those without microembolism. Some of the study limitations could explain this result, such as brain diffusion-weighted MRI only being performed to check for the development of microembolisms in a subset of the participating patients. According to previous studies, microemboli occur in 20-40% of CAS procedures.20,25 Further analyses are needed regarding the impact of microembolisms and different calibers thereof in different brain areas.26 Since the patients who developed microembolisms in the present study suffered a continuous decline in cognitive performance, efforts should be made to minimize the generation of microembolisms by using protective devices during the CAS procedure. The development of microembolisms after CAS is considered to have a greater impact on asymptomatic CS patients than on their symptomatic counterparts.
It was anticipated that patients with chronic perfusion defects would exhibit a greater cognitive improvement after CAS than patients who did not suffer from perfusion defects. However, the results of SVLT and its recognition test demonstrated that their cognitive performance actually declined. This might be because the follow-up test was conducted only 3 months post-CAS, and so the test would not detect long-term recovery of brain function supported by increases in blood flow. Until recently, most of the research on the improvement of perfusion defects and the subsequent recovery of cognitive functions has been based on follow-up tests performed 24 weeks after the CAS procedure. In the future, long-term analyses need to be conducted with brain perfusion imaging and follow-up cognitive performance tests.27
It was expected that the CS location would affect the degree of improvement in cognitive performance, since the left and right hemispheres of the brain play different roles in cognition. However, stenosis laterality had no impact on the degree of cognitive improvement. One caveat to this finding is that neuropsychological tests rarely reflect the cognitive function of the right hemisphere; additional neurocognitive tests, such as the performance intelligence quotient, are needed after CAS to test for hemisphere-dependent improvements.28
This study was subject to some limitations. First, the stent treatment group and the control group were not homogeneous. Second, changes in cognitive performance were observed for a relatively small number of patients over a period of only 3 months, so that occurrence of learning effects cannot be completely excluded. The long-term cognitive function of patients after CAS was not evaluated herein, making it difficult to check and track the development of vascular cognitive impairments or dementia. Third, as mentioned above, brain diffusion-weighted MRI was not performed for all of the patients after CAS due to cost issues, thus failing to check for the development of microembolisms in all CAS-treated subjects. Brain diffusion-weighted MRI was performed for nine of the CS patients, among whom 56.0% were found to have developed a microembolism. This is a relatively high percentage, and may have affected the results of the overall cognitive performance tests. Finally, improvements in cognitive function due to increases in cerebral blood flow must be confirmed by examining functional brain imaging before and after CAS to check for changes in cerebral blood flow.
The findings of this study suggest that CAS exerts beneficial effects on some of the cognitive function of symptomatic CS patients. In particular, symptomatic CS patients exhibited post-CAS improvements in visual memory and overall cognitive function. Future studies should focus on enabling a prognosis and predicting the quality of life of patients undergoing CAS, and to this end should include quantitative measurements of microembolisms, tracking of cerebral blood flow changes, evaluation of long-term standardized neuropsychological tests, and study of the performance intelligence quotient. Furthermore, multicenter, prospective studies should be conducted based on a homogeneous group of patients and should include a control group.


 XML Download
XML Download