

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Sleep problems are common in Alzheimer's disease (AD) patients as well as cognitively normal elderly. Rebok et al.1 reported that 21% of 108 patients with AD experienced sleep disturbances, including frequent awakening, excessive daytime sleepiness, and napping. Community-based cross-sectional studies have found sleep problems in up to 40% of AD patients,2,3 and Moran et al.4 reported that 24.5% of AD patients experienced sleep problems and suffer from delusions, aggression, and other behavioral symptoms during the night. Furthermore, sleep disturbances and nighttime behavior changes are the most important factors in institutionalization of dementia patients.4,5,6,7
It is well known that sleep affects memory and other cognitive functions. Therefore, sleep problems are one of the important factors underlying cognitive decline not only in the normal elderly but also in AD patients.8 In a study of normally cognitive Italian elderly that used patient interviews and the multiple sleep latency test (MSLT) to evaluate nighttime sleep problems and excessive daytime sleepiness (EDS), a significant association was found between these parameters and both dementia and cognitive decline.9 Several reports have been published on the association between sleep problems and cognitive functions in AD.8 A study that administered the Epworth Sleepiness Scale and the Mini-Mental State Examination (MMSE) found that AD patients with greater EDS had lower MMSE scores.10 In another study, shortening of mean daytime sleep latency, identified by the MSLT, was found to be significantly associated with poor MMSE performance, frontal executive function, and verbal memory in both mild and moderate AD.11
The influence of sleep problems on the behavioral and psychological symptoms of dementia (BPSD) in AD has also been studied. One study concluded that sleep disturbance is a predictive factor of depressive symptoms in AD, and another study (that used actigraphy) revealed an association between apathy and sleep problems in AD.12,13 Furthermore, a study performed using the Behavioral Pathology in AD Scale questionnaire found that sleep disturbance in AD was correlated with aggressiveness.4
However, many previous studies on cognitive functions in AD have focused on EDS as the key sleep problem, and not sleep problems at night.9,10,11 Actually, few studies have addressed the effects of nighttime sleep problems on cognitive functions in AD. Furthermore, the previous studies that have been published on this topic used insufficient neuropsychological tests, such as only the Clinical Dementia Rating Scale and/or MMSE, or non-validated patient interview questionnaires.4,7,9,13,14,15,16 Therefore, in the present study we investigated associations between nighttime sleep problems, and cognition and BPSD using detailed neuropsychological tests and a validated sleep questionnaire-comprising the Seoul Neuropsychological Screening Battery (SNSB), the Neuropsychiatric Inventory (NPI), and the Pittsburgh Sleep Quality Index (PSQI) in AD patients.
Methods
Participants
The study population was recruited at the dementia clinic of a South Korean university. The 117 subjects who were enrolled comprised 63 AD patients and 54 age- and sex-matched non-demented elderly (NDE) subjects. AD was diagnosed as described by the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association.17 The NDE subjects included 42 subjects with mild cognitive impairment (MCI) and 12 normal healthy elderly. Diagnostic evaluations included detailed medical history-taking, physical and neurological examinations, neuropsychological tests, and blood tests. The following exclusion criteria were applied: history of significant head trauma, history of neurological disorders, major psychiatric disorders, use of psychoactive medication, and history of abuse of alcohol or another substance. This study was approved by the institutional review boards of all participating hospitals, and written informed consent was obtained after providing a complete description of the study to the subjects and their caregivers.
Global sleep quality
The detailed profiles of nighttime sleep problems experience by AD patients were investigated using the PSQI. This index, which was first introduced in 1988, is a widely used validated sleep scale and is based on a self-assessment questionnaire that assesses sleep problems that have been present during the previous month.18 The Korean version of the PSQI (PSQI-K) used in this study was validated and shown to be reliable in 2012.19 The PSQI consists of 19 items, which generate a 7-component score for subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The total PSQI score can range from 0 to 21, where a higher score indicates a worse sleep quality, and a patient with a total score of ≥5 is considered a poor sleeper.18 We estimated time in bed (TIB) using PSQI subitems. When subjects completed the questionnaire, they were asked to provide the usual times that they went to bed at night and woke up in the morning during the previous month, from which we calculated the usual average TIB of the subjects.
Neuropsychological tests
All study subjects underwent neuropsychological testing using the SNSB.20 This is a standardized neuropsychological battery that contains tests for attention, language, praxis, parietal function, visuospatial function, verbal and visual memory, and frontal executive function. The SNSB consists of digit span (forward and backward), the Korean version of the Boston Naming Test (K-BNT), ideomotor praxis, the Rey-Osterrieth Complex Figure Test (RCFT; composed of copying, immediate and 20-min delayed recall, and recognition), the Seoul Verbal Learning Test (SVLT; 3 learning-free recall trials involving 12 words, a 20-min delayed recall trial of these 12 items, and a recognition test), the phonemic and semantic Controlled Oral Word Association Test (COWAT), and the Stroop test (word and color reading of 112 items over a 2-min period). General cognitive indices were determined using the Korean version of the MMSE.21 The Geriatric Depression Scale was administered to assess depressive symptoms.22,23 BPSD in AD was assessed using the Korean version of the NPI (NPI-K).24
Activities of daily living scales
The Barthel Activities of Daily Living Index (B-ADL) and the Seoul-Instrumental Activities of Daily Living Scale (SI-ADL) were used to evaluate basic activities and instrumental activities of daily living, respectively.25,26,27 A lower B-ADL score means greater impairment of physical ADL, whereas a higher SI-ADL score means greater impairment of instrumental ADL.
Statistics
Statistical analysis was performed using SPSS version 17.0 (SPSS Inc., Chicao, IL, USA) for Windows. Differences between the baseline characteristics of the AD patients and NDE were assessed using the unpaired, two-tailed Student's t-test. Pearson's correlation coefficients and significance levels were used to evaluate correlations between cognitive function, BPSD, and sleep problems. The level of statistical significance was set at p<0.05. A multivariate general linear model adjusted for age and education duration was used to analyze relationships between cognition, BPSD, and sleep problems.
Results
Demographic factors
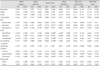
No significant differences were observed between the AD and NDE groups in terms of age, sex, education duration, or total PSQI-K score (Table 1). Poor sleepers (PSQI-K total score ≥5) constituted 40.2% of the AD group and 48.1% of the NDE group. In AD, PSQI-K total scores were not significantly correlated with MMSE-K, B-ADL, or SI-ADL scores. No significant intergroup differences were observed in the components of the PSQI-K between the two groups, except for sleep duration (p=0.002) and TIB (p=0.01) being significantly longer in AD patients than NDE subjects.
Eight of the 64 AD patients reported that they were taking sleeping medications; 5 were taking these 3 or more times a week, and 3 were taking them less than once a week. In the NDE group, four subjects were taking sleep medications three or more times a week, one subject was taking them once or twice a week, and one subject was taking them less than once a week.
Sleep parameters and cognition
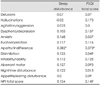
In AD patients, sleep latency was negatively correlated with praxis and visuospatial functions (Table 2). Sleep efficiency was positively correlated with K-BNT, praxis, and RCFT scores. Sleep duration also influenced praxis in AD patients. After adjusting for age and education, sleep latency was significantly associated with praxis, immediate recall, and recognition of the RCFT (Table 3), and sleep duration and efficiency were correlated with praxis in AD patients. Although sleep efficiency appeared to be correlated with K-BNT and RCFT scores, the correlations did not reach statistical significance. The TIB was longer in the AD group than in the NDE group, but no correlation was found between TIB and cognition in AD. No significant difference was found for any cognitive test when the AD group was dichotomized according to TIB (>6 hours vs. <6 hours).
In the NDE group, TIB and daytime dysfunction were negatively correlated with SNSB performance (Table 2). In particular, a longer TIB was associated with worse performance at delayed recall of SVLT, contrasting program, all RCFT components, and COWAT. Daytime dysfunction was also negatively correlated with the COWAT supermarket and Stroop tests. The correlations between TIB, daytime dysfunction, and performance of SNSB were statistically significant in multiple regression analyses controlling for age and education (Table 4).
Sleep parameters and BPSD
In AD, although no significant correlation was observed between PSQI-K total scores and NPI-K scores, sleep disturbance and PSQI-K total scores were significantly associated with apathy/indifference in AD (Table 5). Furthermore, the significant associations between sleep disturbance, PSQI-K total score, and apathy/indifference were preserved after controlling for age and education (Table 6).
Discussion
In this study, poor sleepers (defined by PSQI ≥5)18 constituted 40.2% of the AD group and 48.1% of the NDE group. Not all of the NDE subjects were cognitively normal elderly; there were also some subjects with MCI and subjective cognitive impairment. Thus, the higher prevalence of poor sleepers in the NDE group than in the AD group might have been due to the heterogeneous composition of the NDE group. Based on our data, the prevalence of sleep problems among AD patients was similar or slightly higher than has been reported previously. A community-based study found that 40% of patients with moderate AD have a sleep problem.2 In another report, 35% of AD patients experienced disrupted sleep more than once a week,3 and a recent study of 215 AD patients found that the prevalence rate for sleep disturbance was 24.5%.4 These variations in the reported prevalence rates of sleep problems in AD might be due to methodological differences between studies, such as the types of assessment tools and questionnaires used for evaluating sleep disturbance. In addition, some patients could not complete the questionnaires on their own due to the characteristics of the disease, and thus needed the help of caregivers. We observed that the TIB was longer in AD patients than in the NDE. A similar finding has been reported previously, whereby AD patients had earlier bedtimes and later wake-up times compared to those of a normal control group.10 These differences were considered to be caused by disturbances of sleep/wake rhythms in AD patients.28,29
The main findings of this study were as follows: 1) sleep problems are significantly correlated with cognition in AD, 2) sleep problems are associated with BPSD, and especially apathy/indifference in AD, and 3) TIB is a significant factor that affects cognitive function in NDE but not in AD.
Several studies have produced relatively consistent results regarding sleep duration and cognition, which concur with our results. In a study of elderly subjects with normal cognitive function, Ohayon and Vecchierini.30 reported an association between short sleep duration and both attention-concentration deficits and disorientation in older subjects. In another study conducted on cognitively normal elderly women, the group with <5 hours of sleep had lower cognitive functions than the group with >7 hours.15 That study assessed cognitive functions using a telephone adaptation of the MMSE, verbal memory, category fluency, working memory, and attention tests. In addition, a recent study involving an elderly population aged over 65 years showed that sleeping for less than 6.5 hours/day increased the risk of cognitive decline within a 10-year period.31
While several studies have evaluated associations between sleep profile and cognitive functions in normal elderly populations, few have addressed associations between detailed nighttime sleep profiles and individual cognitive domains. This is due to most studies using daytime sleepiness as a parameter for sleep problems in AD. Lee et al.10 reported that AD patients with severe EDS have lower MMSE scores and a worse functional status as assessed using the Lawton and Brody scale. A study of patients with mild-to-moderate AD using the MSLT concluded that a shorter mean sleep latency was associated with greater impairment of cognitive functions, such as general intellectual and abstractive abilities, verbal memory, language, and praxis, and with lower MMSE scores.11
The findings of the present study show that in AD, longer sleep duration, better sleep efficiency, and shorter sleep latency are correlated with good praxis. Furthermore, a longer sleep latency was found to be associated with impaired visuospatial function. In addition, although sleep efficiency was not significantly related to language function (as assessed using the K-BNT), there was a tendency toward a positive correlation. These results are similar to those of previous studies on sleep problems and cognition. However, the previous studies of AD focused on EDS as a sleep problem, and were thus limited in terms of their abilities to assess nighttime sleep problems.9,10,11 Even studies that used objective tools such as polysomnography assessed the sleep pattern only during a single night.7 In addition, most previous studies used relatively simple tests to assess cognitive functions, whereas in the present study we used detailed and extensive neuropsychological tests.
In the present study, sleep disturbance and total PSQI-K scores were correlated with apathy/indifference in AD patients. Similar results have been reported previously for apathy and sleep problems in AD. One study found that the degree of sleep disturbance was greater in AD patients with apathy than in those without apathy.13 Furthermore, in that study, which used actigraphy, it was found that the AD patients with apathy had a higher percentage of wake after sleep onset, a longer TIB, and decreased daytime motor activities than those without apathy. Another study that used actigraphy found that the daytime mean motor activities were significantly worse in AD patients with apathy than in patients without apathy.16 These previous findings, which are based on the use of objective tools, strengthen the results of our present research.
In the present study, TIB was longer in AD patients than in NDE subjects; however, there was no relationship between cognition and TIB in AD. These results differ from those of a previous study in which a longer TIB was associated with worse cognitive function in AD, but not in NDE.32 That study observed a negative association between TIB and MMSE in AD patients, and that the patients with a TIB of >6 hours performed worse in the MMSE and ADL tests than patients with a TIB of <6 hours. However, this difference could have been due to the patients with a TIB of >6 hours being older. On the other hand, there was no age difference between the AD and NDE groups in the present study, and we found no such differences when we dichotomized AD patients about a TIB of 6 hours. A particular interesting finding in the present study was of a significant negative correlation between cognition and TIB in the NDE group. It is possible that an association exists between nighttime insomnia and daytime cognitive decline, because a longer TIB means insomnia at night, which could influence daytime cognition among NDE.33 On the other hand, it could be that the TIB effect was masked by existing cognitive decline in AD. However, TIB was calculated based on the results of a subjective questionnaire and not objectively using, for example, actigraphy, and our NDE group included MCI patients. This topic clearly requires further investigation.
The interpretation of our results is limited by the modest size of our study population. Furthermore, although all of the study subjects were instructed to complete a questionnaire on their own, it is likely that AD patients received help from caregivers because of the characteristics of the disease. It is possible that the caregivers did not report sleep problems unless their own sleep was disturbed, and that the answers given were influenced by the caregivers' perceptions. This constitutes a major weakness of questionnaire-based studies on sleep disturbance in AD. In addition, even though no specific difference was observed in the sleep/cognition relationship between MCI and normal elderly in our preliminary analysis, some of the NDE subjects in this study had MCI. Therefore, further studies are required using large healthy normal control groups.
In conclusion, the findings of this study suggest that night-time sleep is important for cognitive function and BPSD in AD. Therefore, sleep problems should be considered when treating AD patients because their treatment might improve both cognitive function and BPSD.




 XML Download
XML Download