

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Dermatologists may encounter unexpected complications after skin biopsy. Cook and Perone1 prospectively examined dermatologic surgical complications in the office setting, and overall complication rate of 1.64% in 1,343 cases were found, most of which was minor difficulties with hemostasis. Vascular complications rarely occur in dermatologic outpatient based procedures. It is thought to be especially rare after punch biopsies with relatively small and superficial incision. Complications of this category include post-biopsy bleeding, slowly developing chronic expanding hematoma2 and rarely pseudoaneurysm3. Here, we report a case of pseudoaneurysm after punch biopsy which spontaneously subsided.
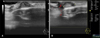
A 62-year-old man visited us with complaint for a 1×1.1-cm-sized pulsating mass on the right temporal area (Fig. 1). He had taken 4 mm punch biopsy on same area under the suspicion of verruca vulgaris 2 weeks ago. In past medical history, he was being treated for the right cerebral infarction and was on warfarin 5 mg and acetylsalicylic acid 100 mg daily at the time of biopsy. Hematoma was clinically suspected and we decided to closely follow-up the patient. However, the lesion did not decrease in size after 3 months of follow-up visit, and we performed ultrasonography on the protruded site. The ultrasonography revealed mixed-echoic subcutaneous lumen and connected fistula without increased blood flow (Fig. 2). Pseudoaneurysm which occurred on the superficial temporal artery branch was clinically suspected and we planned to incise and ligate the artery. However, the patient refused the procedure and wanted to observe the lesion for the time being. It became pulseless and gradually began to flatten after 5 months. The lesion had spontaneously subsided and no further recurrence was seen to this day.
Pseudoaneurysm is a well-known sequela of trauma and iatrogenic injury of the superficial temporal artery and consists of an organized hematoma that communicates with the injured artery via a sinus tract. It develops when trauma disrupts the arterial wall and blood pressure from the artery exceeds the capacity of the coagulation cascade. The hematoma may canalize and remain in persistent communication with the lumen of the artery. Most reported cases on the face occurred on the superficial temporal artery and its branches owing to its superficial course above the skull surface4. Suture ligation of the implicated artery is traditionally considered the treatment of choice5.
Here, we report a unique case of pseudoaneurysm occurred after punch biopsy on the right temporal area with spontaneous remission. Dermatologist should keep in mind that this rare complication can be encountered even after small trauma such as punch biopsy. Especially, in case of performing biopsies in the temporal area, dermatologists should keep the predictable course of the superficial temporal artery in mind. Moreover, if such complication occurs, the possibility of spontaneous remission, as in our case, can be considered before initiating surgical treatment.

 XML Download
XML Download