

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) manifests as chronic relapsing eczema of the skin, showing a typical pattern on specific locations, depending on the patient's age. Among various instruments for AD diagnosis, the International Study of Asthma and Allergies in Childhood (ISAAC) is considered as a standard tool for cross-sectional, epidemiological surveys of childhood AD, and it has been used and validated worldwide since 1990s up till now123. AD prevalence among children is approximately 10%~20%, but AD prevalence among adults decreases later to less than 5%, indicating that many AD patients have a good prognosis and can remit spontaneously during their lives4567. Spontaneous remission of AD was reported to occur before adolescence in 40%~70% of patients with infantile AD89. In epidemiological surveys by using the ISAAC-based questionnaire, the one-year AD prevalence in childhood was reported to be 19.1% (in 2008) in Korea10.
As for the onset, AD is known to develop commonly during the very early stage of life: approximately 50% of patients develop AD before 2 years of age, and a majority of patients develop AD by 5 years of age11. On the same basis, the U.K. Working Group's criteria for AD diagnosis include one item of ‘early onset before 2 years’ among the five-item criteria1213. Recently, however, the prevalence of late onset AD is increasing worldwide, and it has been reported that almost half of patients developed AD from juvenile stage (unpublished data). These results suggest that continuous monitoring of AD prevalence in given communities or individuals is very important for efficient AD management.
Due to inherent limitations of the ISAAC as a diagnostic tool for follow-up studies at an individual level, there is no report on the age-dependent change in AD prevalence via sequential follow-up studies on childhood AD in a community setting10. Instead, the age-dependent change in AD prevalence has been reported by studying infantile AD patients who visited hospitals or were admitted to hospitals for their skin conditions, or children who were diagnosed with AD at hospitals, and not by community-based surveys891415. Hospital-visiting AD patients are known to have more severe symptoms than those detected by field surveys. In previous reports about severity of AD, 67.9%~86.1% of AD cases were mild in community-based surveys, but 32.7% of AD cases were mild in hospital-based surveys15161718. Moreover, 36% of schoolchildren with AD in a community had not consulted their doctors, probably because the disease was mild18. Therefore, the generalization of results from hospital-based surveys to the whole population in a given community contains a high probability to cause selection bias.
With this background, this study aimed to evaluate the age-dependent change in AD prevalence among children in the age range of 7~8 years at an individual level. In this study of a community-setting, skin examination by dermatologists, instead of questionnaire-based survey, for AD diagnosis was used.
MATERIALS AND METHODS
Study population and study design
Children aged 7 to 8 years in 2011 who were in the elementary school of Gwangju, Korea were recruited. A total of 305 children were included, and they were followed up at twice a year (June and December). Both skin examination by dermatologists was performed prospectively for 4 years. From 2011 to 2014, 32 children dropped out, and a total of 273 children were followed up (Fig. 1). In 2011, the number of children who were 7 years and 8 years of age was 119 and 154, respectively. There were 146 boys (53.5%), and 127 girls (46.5%). The study was approved by Chonnam National University Hospital Institutional Review Board (IRB no. CNUH-2012-099) and conducted according to the ethical guidelines of the Declaration of Helsinki.
Gold standard for the AD diagnosis
One-time skin examination is likely to exclude mild or transient AD cases, in which many AD children with mild symptoms showed a temporary remission for certain time periods in a year19. Therefore, as a gold standard for AD diagnosis, skin examination by dermatologists should be performed twice a year at least in the same group of children. Two dermatologists visited the elementary school for skin examination. Considering that there are two seasons (summer and winter) in which AD symptoms can be aggravated in Korean AD children (unpublished data), we performed the 1st skin examinations in June. Based on the results of the skin examination, children were classified into one of the three groups; ‘AD’, ‘non-AD’, and ‘undetermined’. In December, the 2nd skin examination was performed in children, who were classified as ‘non-AD’ and ‘undetermined’ on the 1st skin examination. When AD was diagnosed at least once in June or December, it was defined as presenting AD during that year. The severity of AD was graded as mild, moderate, or severe according to the following criteria: (1) mild, skin involvement by mild eruption only; (2) moderate, <10% surface area involvement by severe eruption; (3) severe, >10% of body involvement by severe eruption18.
Definition of spontaneous remission
Decision between the ‘spontaneous remission’ group and the ‘intermittent or persistent’ group was taken in 47 children who were diagnosed with AD in 2011. We defined ‘spontaneous remission’ in AD children who were disease free for 3 years continuously: skin lesions were not detected on skin examinations by dermatologists, twice a year. If children did not satisfy the above requirements, they were classified into the intermittent or persistent group.
Statistical analysis
Pearson's chi-squared test was used for analyzing the factors associated with remission of AD. The factors included age, aggravation due to food, and family history of asthma, allergic rhinitis, allergic conjunctivitis, AD, and atopic diseases. Atopic diseases were classified as diseases including asthma, allergic rhinitis, allergic conjunctivitis, and AD. IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) was used to analyze the data, with p-values of <0.05 being considered statistically significant.
RESULTS
Spontaneous remission of AD
Of the 47 children who were diagnosed with AD in 2011, nine patients (19.1%) showed spontaneous remission, and 38 patients (80.9%) had intermittent or persistent symptoms during the 4 years follow-up period. Two hundred thirteen children who did not show any symptoms during the follow-up period were classified into the non-AD group (Fig. 1).
Change in AD prevalence
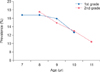
A total 5.9% decrease in AD prevalence was observed during the 4 years follow-up period. The annual change in prevalence among first graders was 16.8% (7 years of age), 16.8% (8 years of age), 15.9% (9 years of age), and 12.6% (10 years of age). The annual change in prevalence among second graders was 17.5% (8 years of age), 14.9% (9 years of age), 13% (10 years of age), and 10.4% (11 years of age) (Fig. 2).
Onset age and severity of AD
Additional questionnaire-based surveys on the onset age and aggravating factors were performed for children who were diagnosed as AD by skin examination. The onset age was ≤1 year in 24 patients (40%), 2~3 years in 19 patients (31.7%), and ≥4 years in 17 patients (28.3%). Thirteen children (21.7% of AD patients) had AD after 8 years of age, or were diagnosed with AD on skin examination during our study (Fig. 3). The severity of AD was mild in 33 out of the 47 AD patients (70.2%), moderate in 13 AD patients (27.7%), and severe in 1 AD patient (2.1%) in 2011 (Table 1).
Factors associated with spontaneous remission of AD
Forty-seven children, who were diagnosed as having AD in 2011, were classified into the ‘spontaneous remission’ group and the ‘intermittent or persistent’ group. Family history of atopic diseases, which include asthma, allergic rhinitis, allergic conjunctivitis, and AD, was positive in 38 patients (80.9%). Sex, family history of asthma, allergic rhinitis, allergic conjunctivitis, AD, and atopic diseases did not show a statistically significant difference between the ‘spontaneous remission’ group and the ‘intermittent or persistent’ group (Pearson's chi-squared test, p>0.05) (Table 2).
DISCUSSION
AD is a common inflammatory skin disease in childhood, often manifesting in early infancy and has a natural course that varies over time. One of misconceptions among parents of children with AD is that AD is a life-long persistent disease, although this is true only in a small number of patients14. Lack of information about the natural course causes anxiety, and leads to the use of an unscientific approach and untested regimens. Because the natural course of AD varies among individuals, studies on its natural course in different age groups and races are important. However, because only few prospective studies exist, the natural course of AD is not completely known. Most epidemiologic studies of AD are cross-sectional studies showing point prevalence, and it is difficult to understand the natural course of AD2021. Previous studies have been flawed because only the patients with infantile AD in a hospital setting are considered1122. The results do not reflect the other age groups of AD except for infantile AD. Furthermore, there is a large difference in severity between patients in a hospital setting and those in a community setting. The proportion of patients with severe AD in a hospital setting is higher than that of patients with severe AD in a community setting23. The previous study in Koreans has a limitation in terms of its retrospective nature, and it was performed by reviewing the medical records and parents' telephone interview14.
In previous studies, about 70% of infantile AD cases went into spontaneous remission91415. In a population-based cohort study from Taiwan, spontaneous remission occurred in 69.8% of the 1,404 early-onset AD patients (onset in the first 2 years) during the 10-year follow-up period9. In a study, which was performed for 5 years in children in the age group of 1~3 years , 52% showed spontaneous remission24. In a study, which was performed in children in the age group of 9~11 years until they were 16 to 20 years old, 6.1% showed spontaneous remission25. In previous studies, the spontaneous remission rate was decreased significantly with aging. In this study, children in the age group of 7~8 years were followed up prospectively until they were 10~11 years old, and spontaneous remission was detected in 19.1% of patients. This result reflects the natural course of childhood AD in 7 to 11 years old children who had not been included in previous studies.
In a previous sequential study on AD prevalence in the same group (19% in the 0 to 1 year age group, 14% in the 1 to 2 years age group, and 5% in the 6 to 7 years age group), spontaneous remission of AD was commonly observed in the early stage AD patients9. In this study, we found that the change of AD prevalence in children of the 7~8 years age group (0.9%~3.3% decrease every year) was markedly lower in comparison with that in children of the 0~1 year age group9. These results reflect the importance of surveys in children of different age groups in relation with spontaneous remission of AD in the future.
Due to the difference in the population, the factors associated spontaneous remission of AD were inconsistent with those in previous studies9152224. One study in Europe showed that the course of AD is significantly related to egg sensitivity, and the average healing time is higher in egg-sensitive patients15. The other study showed that independent factors at baseline predicting remission were milder type, later onset, non-flexural area, no food allergy, and rural living24. However, a population-based cohort study from Taiwan in 1,404 AD patients showed that sex, onset age, presence of allergic rhinitis, presence of asthma, and presence of respiratory atopy (either allergic rhinitis or asthma) did not have a statistically significant influence on disease course9. A meta-analysis study about the factors predicting complete remission showed that parental allergy and sex did not predict the remission of infant-onset AD until the age of 6~7 years22. A retrospective study in Korean AD patients showed that none of the risk factors were significant by multivariate analysis, but maternal diet restriction during lactation and no sensitization to cow's milk were significantly associated with remission of AD in the moderate-to-severe AD group14. In this study, sex, family history of asthma, allergic rhinitis, allergic conjunctivitis, and AD did not show a statistically difference between the spontaneous remission group and the intermittent or persistent group. This result was in accordance with the previous reports91422, which did not show any factors associated with remission when the population had a high proportion of mild AD cases.
Most of the AD patients are diagnosed before childhood especially in the first year of life2627. One questionnaire-based survey of 7~8 years old Korean children reported the following findings: onset age: <2 years in 43.7% and ≥5 years in 26% of children21. However, the prevalence of late-onset AD or relapsing AD that shows re-occurrence of AD symptoms after pubertal age is increasing worldwide. Almost half of the patients developed AD from the juvenile stage; juvenile stage (10%), early adult stage (13%), late adult stage (20%), and senile stage (1%~3%) (unpublished data). The onset age was found to be 10% in <2 years old children, 28.3% in ≥5 years old children, and 21.7% in >8 years old children, showing an increase in the prevalence of late-onset AD. These patients were diagnosed with AD by skin examination performed by dermatologists which might be more precise than the questionnaire survey.
This study has several advantages over previous studies. Firstly, our prospective study was performed for four years. For reducing the error in AD diagnosis, skin examinations were performed twice every year (June and December) by dermatologists. Secondly, the age-group for this study was 7~11 years and this age group had not been studied in previous reports. Thirdly, our study was a community-based survey that more precisely reflected the course of mild AD (70% of total AD children) in a population-based setting. However, this study has limitation, because it was done in small population (n=305). Further studies are required to unravel the true prognosis of childhood AD in Korea by a large-population-based survey for longer follow-up periods. The recall bias could be in this study, because the questionnaire survey was done for aggravation factors of AD.
This study was a community-based follow-up study about the natural course of childhood AD (7 to 11 years of age) in Gwangju province, Korea. The population was selected from a community, not from a hospital, and the study was performed prospectively. We found that 19.1% of AD patients showed spontaneous remission, and 80.9% of AD patients had intermittent or persistent symptoms during the 4 years follow-up period. A total decrease of 5.9% in the AD prevalence was noted in the 4 years follow-up period. Also, 21.7% of patients developed AD after 8 years of age or were diagnosed by skin examination during our study. Sex, family history of asthma, allergic rhinitis, allergic conjunctivitis, AD, and atopic diseases did not show a statistically difference between the spontaneous remission and intermittent or persistent groups.



 XML Download
XML Download