

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Segmental neurofibromatosis 1 (NF1) is generally accepted to be the result of somatic mosaicism for a NF1 mutation that occurs early in embryogenesis. Segmental NF1 is roughly 10 times less frequent than NF1. This condition is characterized by the typical features of NF1 that are limited to a specific body segment1. The distribution is usually unilateral; however, bilateral occurrences have been reported2. Although deep-seated neurofibromas have been occasionally reported in generalized NF1, extracutaneous manifestations in segmental NF1 have rarely been reported3.
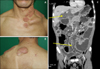
A 45-year-old Korean man visited the emergency department in our medical center with signs of an acute abdomen. The history and physical examination revealed a 35-year history of multiple, soft-to-firm, asymptomatic, flesh colored plaques and nodules on the left side of neck, shoulder and upper back (Fig. 1A, B). The plaques had gradually increased in size over time. He had several café-au-lait macules, but no skin-fold freckling. His medical history and family history were non-contributory. The ophthalmologic examination revealed Lisch nodules on both the irises.
A contrast-enhanced computed tomography (CT) was performed of the chest and abdomen and revealed diffuse, infiltrative skin and subcutaneous masses. Furthermore, low attenuated masses were also seen in the retroperitoneal space, porta hepatis and small bowel mesentery, and mediastinum (Fig. 1C). The diagnostic laparoscopy revealed multiple nodules in the intraperitoneal space. A resection of the visible nodules in the mesentery of the small bowel was performed for biopsy. The brain CT revealed normal findings. The patient did not undergo any other additional therapy.
The histological analysis of the nodules from the skin and the mesentery of the small bowel revealed nodular infiltration of fusiform cells and the presence of oval and fusiform shaped nuclei that formed strands crossing each other. The immunohistochemical examination showed positive staining with S-100 protein.
In 1987, Roth et al.4 suggested that segmental neurofibromatosis should be separated into four different subtypes. Roth's classification type II was defined as non-familial and segmental neurofibromatosis with deep systemic involvement as in our case.
The frequency of deep-seated neurofibromas in NF1 has been reported to be 44% in abdomen/pelvis and 20% in thorax, respectively1. In contrast to NF1, systemic involvement in segmental NF1 is uncommon3 and the incidence of visceral neurofibromas in segmental NF1 is unknown.
Since gastrointestinal neurofibromas are rare, a high degree of suspicion is needed for timely diagnosis. Generally, delay and difficulty arises in the diagnosis of gastrointestinal neurofibromas, due to the presence of non-specific symptoms as well as the predominantly small bowel location5. In our case, the patient reported abdominal pain, but during the laparoscopy the physicians did not observe any other specific findings except for the intra-peritoneal neurofibromas. Consequently, we suspected that the patient had symptomatic intra-abdominal neurofibromas. Surgical excision is the treatment of choice for all symptomatic tumors occurring in patients with NF1, and it may be the same in segmental NF1. However, surgical excision of benign asymptomatic tumors is still controversial.
In conclusion, we report a rare case of segmental NF1 with intra-thoracic and intra-abdominal neurofibromas. To our knowledge, this is the first such case report in Korea. If patient with segmental NF1 complains of non-specific abdominal pain, visceral neurofibromas should be considered.
 XML Download
XML Download