

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Melkersson–Rosenthal syndrome (MRS) is an uncommon disease with unknown etiology characterized by recurrent orofacial edema, relapsing facial paralysis, and fissured tongue. Noncaseating epithelioid granuloma was a main histopathologic feature12. In patients with MRS, other sites beyond the orofacial region are very rarely reported. Here, we presented one boy diagnosed with MRS with genital swelling, and reviewed related literatures.
CASE REPORT
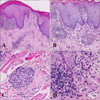
A 12-year-old boy presented with relapsing swelling of the lower lip and penis for 2 years and right facial paralysis for 20 days. He had no respiratory or gastrointestinal problems and denied any history of allergy, irritants contact, local trauma, or infection. Physical examination showed localized swelling of the lower lip with slight crust and fissure on the surface (Fig. 1A), deep fissures in the dorsum of the tongue (Fig. 1B), and cobblestone-like hypertrophy of the buccal mucosa. A droop of mouth angle and a shallower nasolabial groove on his right face were noted (Fig. 1C). No oral ulceration or gingival hyperplasia was observed. His penis showed a circumscribed edematous patch with mild crusts (Fig. 1D). The results of the rest of his physical examination were unremarkable, and there was no similar record in his family.
Laboratory tests revealed slightly elevated lymphocyte counts (5.3×109/L) and immunoglobulin E level (114 IU/ml). Electromyography of the right peripheral facial nerve showed delayed motor conduction and decreased amplitude, suggesting nerve fibril damage. Results of other routine tests—including erythrocyte sedimentation rate, C-reactive protein, antistreptolysin O, rheumatoid factor, antinuclear antibody, serum immunoglobulin (IgA, IgM, IgG), complement components (C3, C4, and C1 inhibitor), allergen detection, and chest radiogram—were all either within normal ranges or negative.
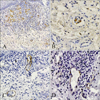
Examination of skin biopsy specimens from the lower lip and penis showed identical histological changes. The epidermis showed mild hyperkeratosis, parakeratosis, and acanthosis with scattered vacuolar degeneration of basal cells and epidermotropic lymphocytes. Several well-formed noncaseating granulomas were distributed throughout the dermis, and most of them surrounded or filled into dilated vessels (Fig. 2). A large number of CD68-positive histiocytes were crowded in the granuloma region (Fig. 3A), and some of them were even located only within dilated vessels (Fig. 3B). Immunohistochemical D2-40 staining showed that most of the affected vessels were lymphatic vessels (Fig. 3C); blood vessels marked by CD31 were normal size; and no granulomas were detected in their cavities (Fig. 3D).
All 12 exons of the CARD15/NOD2 gene extracted from the patient's peripheral blood were also sequenced and analyzed, and only one single nucleotide polymorphism was found: rs1861759 (c.1761 T>G; R587R), which indicated a single nucleotide polymorphism mutation.
The boy was diagnosed with MRS and treated with oral methylprednisolone 8 mg per day and topical 0.03% tacrolimus cream. The two lesions improved after 3 months of therapy, and then oral methylprednisolone was tapered and stopped after 6 months. Topical tacrolimus cream and oral thymosin were used as a maintenance regimen since then. There was significant improvement on his lower lip (Fig. 1E) and penis (Fig. 1F), and no symptoms or signs of other systemic diseases (Crohn's disease [CD] or sarcoidosis) were observed during the 2 years of follow-up.
DISCUSSION
MRS is an uncommon granulomatous disease. The diagnosis of MRS is often difficult because the complete triad is reported in only 8% to 18% of MRS123, whereas granulomatous cheilitis without facial paralysis—also called incomplete MRS—is more common.
The most common manifestation of MRS is nonpitting swelling in the orofacial region, and the upper lip is the most frequently involved site; the lower lip is less frequently involved4. Intraoral signs include swelling of gingival and mucosa, fissured tongue, and ulceration234. Recurrent genital swelling in either complete or incomplete MRS is very rare; we found only 11 suspected cases reported in the literature (Table 1)56789101112131415. Genital swelling in MRS is similar to orofacial swelling in clinical features and pathological changes13. Patients generally presented with painless, circumscribed, and firm edema in the anoperineal region. It is worth noting that half of those cases were complicated with CD, and actually, whether MRS and CD belong to the same disease spectrum has long been controversial.
CARD15, originally named NOD2, was the first identified susceptibility gene of CD. Recent studies showed it was also associated with other systemic granulomatous diseases like Blau syndrome and early-onset sarcoidosis16. CARD15 was essential for innate immunity and control of inflammation, and when dysregulated, it caused inflammation disease via aberrant activation of NF-κB and mitogen- activated protein kinase pathways and played a pathogenic role in the formation of granulomas16. MRS shared many clinical and pathological similarities with other granulomatous diseases, whereas Gale et al.17 reported that MRS and CD were genetically different because none of the 17 Swedish patients with complete or incomplete carried any CD-linked CARD15 variation. In our case, we found just one single nucleotide polymorphism— c.1761 T>G (R587R)—which indicated that CARD15 was not involved in the pathogenesis of the patient. The boy had no gastrointestinal symptoms, his fecal occult blood test was repeatedly negative after 2 years of follow-up, and he had typical clinical triad symptoms and noncaseating granuloma of MRS; therefore, he was diagnosed with complete MRS with genitalia involved, which had never before been reported in a child.
MRS usually occurs in childhood and adolescence, and its exact etiology remains to be elucidated, although several risk factors, including infection, allergy, hereditary predisposition, autoimmune disorder, and foreign-body irritation, have been discussed in the literature123. The characteristic histopathological finding in MRS is noncaseating granuloma. The granuloma is distributed mainly in the superficial and middle layers of dermis and is composed of histiocytes, lymphocytes, and small numbers of multinucleated giant cells and plasma cells. The pathological mechanism of localized edema in MRS is not well understood. In the boy, we observed intralymphatic granuloma in two lesions, whereby we proposed that lymphatic vessel obstruction and destruction caused by infiltrating granuloma may contribute to localized edema of MRS, which agreed with the results of González-García et al.18.
There is no known satisfactory cure for MRS. Systemic or intralesional corticosteroid is often temporarily beneficial. Immunosuppressive regimens, like clofazimine, dapsone, sulphasalazine, thalidomide, and minocycline, have also been reported to be alternatives to glucocorticoid. Surgery is recommended for severe cases and for patients who cannot tolerate glucocorticoid treatment19.
By presenting our case and reviewing reported MRS with genitalia involvement, we demonstrated that genital swelling as a special complication of MRS should be noticed and that lymphatic obstruction possibly contributes to localized edema.


 XML Download
XML Download