

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A cutaneous premalignant lesion is a lesion that has not yet become invasive skin cancer although these lesions do have the potential to become malignant. The term "premalignant lesion" is occasionally used to describe carcinoma in situ, which is non-invasive cancer that is technically "cancerous" but has not progressed to an aggressive and/or invasive stage. In this context, Bowen's disease (also known as squamous cell carcinoma in situ) is characterized by atypical squamous cells that proliferate throughout the entire epidermis, and this lesion is classified as a cutaneous premalignant lesion, as Bowen's disease is not invasive1. Therefore, the representative cutaneous premalignant lesions are actinic keratosis and Bowen's disease.
The prevalence of malignant skin tumors is increasing, both globally and in Korea, and diagnoses of cutaneous premalignant lesions are also becoming more frequent. Various factors are known to contribute to this increase, including an aging population, an increase in outdoor activities, increased exposure to ultraviolet light due to changes in the ozone layer, easier access to medical services, and an increase in patients' awareness of skin cancer and cutaneous premalignant lesions2. However, while many epidemiological studies have examined the prevalence of malignant cutaneous tumors, epidemiological studies of premalignant lesions are rare. Furthermore, although previous studies among Caucasian populations have provided substantial epidemiological data, including an increase in skin cancer incidence, little is known about the incidence and trends for skin cancers in the Asian populations3.
To date, only a few statistics have been reported regarding the prevalence and incidence of cutaneous premalignant lesions for several regions in Korea and other Asian countries456. Therefore, we retrospectively evaluated a large number of outpatients who had visited a dermatologist at our institution over a 19-year period and identified the patients who were diagnosed with cutaneous premalignant lesions. Using this data, we analyzed the incidence and clinical patterns of cutaneous premalignant lesions in a Korean population and compared our results to the previously reported domestic and international statistics.
MATERIALS AND METHODS
Study targets
Among the 70,867 new outpatients who visited a dermatologist at the Dong-A University Hospital between January 1995 and December 2013, a definite diagnosis of actinic keratosis or Bowen's disease was made for 1,292 patients via histopathological examination. These patients were the study targets, and their medical charts, clinical images, and histopathological findings were retrospectively evaluated. The study was approved by the Institutional Review Board in Dong-A University (14-023).
Study method
To determine the yearly incidences and clinical characteristics of actinic keratosis and Bowen's disease, we analyzed data regarding diagnoses, patient age at the time of diagnosis, sex, tumor location, concomitant skin cancers, occupation-related risk of sun exposure, and number of lesions. Cases were further divided into those with single or multiple lesions, and the average age, occupation-related risk of sun exposure, and concomitant skin cancer incidences were then analyzed and compared to the existing Korean and international statistics.
Statistical analysis
Categorical variables were reported as counts and relative frequencies. Differences in average age (according to single or multiple lesion status) were evaluated using an independent t-test, and differences in occupational-related sun exposure or concomitant skin cancers were evaluated using the Pearson chi-squared test. All analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), and p-values <0.05 were considered statistically significant.
RESULTS
Cutaneous premalignant lesion incidence
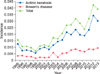
Of the 70,867 new outpatients who visited a dermatologist at our institution between January 1995 and December 2013, 1,292 patients were diagnosed with cutaneous premalignant lesions via biopsy, which corresponded to an average yearly incidence of 1.82%. However, the yearly incidence of patients with at least one cutaneous premalignant lesion ranged from 0.70% to 4.25% over the study period, and the incidences and numbers of new cases increased over this period (Fig. 1).
Incidence according to cutaneous premalignant lesion types
Among the 1,292 cases of cutaneous premalignant lesions, actinic keratosis was the most frequent lesion (980; 75.85%), followed by Bowen's disease (312; 24.14%). During the study period, the average yearly incidences of actinic keratosis and Bowen's disease were 1.38% and 0.44%, respectively, with the incidences of both lesions increasing over time (Fig. 1).
Distribution according to sex and age
Among the 1,292 patients, 512 patients were men, and 780 were women, which corresponded to a male:female ratio of 1:1.52. The male:female incidence ratio for actinic keratosis was 1:1.81, revealing a higher incidence in women. In contrast, the male:female incidence ratio for Bowen's disease was 1.09:1, revealing a slightly higher incidence in men. The average age at the time of diagnosis was 68.76 years (men, 70.89 years; women, 65.56 years). The average age at the time of an actinic keratosis diagnosis was 70.34 years (men, 67.33 years; women, 72.04 years), compared to 64.15 years (men, 62.12 years; women, 66.40 years) for Bowen's disease. Patients who were 70~79 years old had the highest incidence (401; 31.03%), followed by patients who were 60~69 years old (376; 29.10%), 80~89 years old (228; 17.65%), 50~59 years old (151; 11.69%), 40~49 years old (69; 5.34%), 30~39 years old (51; 3.95%), and 90~99 years old (16; 1.24%) (Fig. 2).
Lesion location
In the patient population, cutaneous premalignant lesions were located on the face (1,064; 82.35%), lower limbs (89; 6.89%), upper limbs (42; 3.25%), hands (35; 2.71%), anogenital region (24; 1.86%), feet (12; 0.93%), neck (11; 0.85%), and scalp (9; 0.70%). Actinic keratosis was located on the face (951; 97.04%), hands (18; 1.84%), upper limbs (15; 1.53%), scalp (9; 0.92%), torso (8; 0.82%), neck (6; 0.61%), lower limbs (2; 0.20%), and feet (1; 0.10%). Bowen's disease was located on the face (113; 36.22%), lower limbs (87; 27.88%), trunk (57; 18.27%), upper limbs (27; 8.65%), anogenital region (24; 7.69%), hands (17; 5.45%), feet (11; 3.53%), and neck (5; 1.60%) (Fig. 3).
Associated malignant skin tumors
A total of 204 (15.79%) cases were accompanied by malignant skin tumors, including 115 (8.90%) cases of squamous cell carcinoma (SCC), 83 (6.42%) cases of basal cell carcinoma (BCC), and 9 (0.70%) cases of malignant melanoma. Three patients (0.23%) were previously diagnosed with both BCC and SCC (Fig. 4). For actinic keratosis, 150 (15.31%) patients also had malignant skin tumors, including SCC (8.06%), BCC (6.53%), and malignant melanoma (0.71%). For Bowen's disease, 54 (17.31%) patients also had malignant skin tumors, including SCC (11.54%), BCC (6.09%), and malignant melanoma (0.64%).
Numbers of lesions
A total of 3,651 lesions were diagnosed via biopsy, which corresponded to an average of 2.71 lesions per patient although the majority of patients (59.13%) only had a single lesion. The average number of lesions for actinic keratosis was 3.25 lesions per patient although most patients (53.06%) had a single lesion. The average number of lesions for Bowen's disease was 1.48 lesions per patient although a single lesion (78.21%) was more common than multiple lesions.
1) Average age according to lesion number
The average age of the patients with multiple lesions was 71.52 years, which was significantly higher than the average age of the patients with a single lesion (65.82 years, p<0.001) (Table 1).
2) Risk of ultraviolet exposure according to lesion number
The patients' occupations were determined using their medical charts, and the risk of ultraviolet light exposure was compared between outdoor and indoor workers. Among the 993 patients whose occupations could be determined from their medical charts, 337 (33.94%) patients were outdoor workers. Of patients with multiple lesions, 42.29% of these patients were outdoor workers; this rate was significantly higher than the incidence among patients with a single lesion (28.26%, p<0.001) (Table 1).
3) Concomitant malignant skin tumors
Of the patients with multiple lesions, 24.05% of patients had a history of skin cancers, which was significantly higher than the incidence among patients with a single lesion (10.08%, p<0.001) (Table 1).
DISCUSSION
In the Korean literature, the reported incidence of cutaneous premalignant lesions ranges from 0.06% (1982~1996) to 0.56% (1999~2008)578. In the present study, we found that the cutaneous premalignant lesion incidence was 1.82%, which is higher than the average incidences reported in previous Korean studies. This discrepancy may be explained by the recent increase in cutaneous premalignant lesion incidence. According to Moon et al.9, the skin cancer incidence was 4-fold higher in 1998, compared to that in 1984, while the cutaneous premalignant lesion incidence increased 50-fold, indicating a much faster increase in cutaneous premalignant lesion incidence. Our study also revealed a rapid increase from 0.70% in 1999 to 4.25% in 2012. In addition, the change in ultraviolet exposure according to latitude is believed to have contributed to the high cutaneous premalignant lesion incidence observed in this study because our clinic is located in a southern region of Korea (Busan). According to data from the Korea Meteorological Administration, despite small differences in latitude between regions, the amount of ultraviolet radiation received is variable in Korea2. The size of each region's elderly population is another factor that may contribute to high regional prevalences of cutaneous premalignant lesions. Ha et al.2 has stated that the ratio of elderly to non-elderly persons is highest in Busan (11.26%), compared to Seoul and six other metropolitan areas.
In the present study, the most frequent cutaneous premalignant lesion was actinic keratosis (75.86%), which confirms the results of earlier studies5781011. Although the incidence in this study was higher than the 48.7% that was reported by Chung et al.7, it was similar to many previous Korean reports (67.7%~79.7%)581011. In addition, the average actinic keratosis incidence was 1.38% during the study period. We also found that Bowen's disease comprised 24.14% of the cutaneous premalignant lesions in this study, which was similar to that found in previous Korean reports (19.8%~25.3%)511. Based on this data, the average Bowen's disease incidence during the study period was 0.44%.
The average patient age at the time of diagnosis was 68.8 years (men, 65.6 years; women, 70.9 years) in the present study. In addition, we found that 96.05% of cutaneous premalignant lesions were found in patients who were ≥ 40 years old, and this finding is consistent with previous reports57. Furthermore, the average age at an actinic keratosis diagnosis was 70.37 years, which is similar to that in previous Korean reports (67.6~71.6 years)411. Moreover, the average age at a Bowen's disease diagnosis was 64.2 years, which was similar to that from previous Korean reports (56.5~67.7 years) although it was noticeably lower than that for actinic keratosis.
Furthermore, our observed male:female ratio for these lesions was 1:1.52, and this finding is similar to those that were reported by previous Korean studies (ranging from 1:1.37 to 1:2.48)57811. This sex-related difference may be because women are more likely to visit a hospital upon the early onset of symptoms, leading to a diagnosis at the premalignant stage2. In addition, modern women have increased life expectancy and exposure to sunlight due to increased social and leisure activities, which may also be relevant factors2. Our analysis of cutaneous premalignant lesions according to type revealed that actinic keratosis diagnoses had male:female ratio of 1:1.81, which is similar to those that have been reported in previous Korean studies (ranging from 1:2.0 to 1:2.76)511. Furthermore, the male:female incidence for Bowen's disease was 1.09:1, which is similar to that reported by Park et al.11 (1.9:1) although it is different from that reported by Hong et al.5 (1:1.85).
Cutaneous premalignant lesions were most common in the facial region (82.35%), which is consistent with previous reports5811. The face receives more continuous sun exposure than any other part of the body, and it accumulates more ultraviolet radiation. This fact highlights the close relationship between cutaneous premalignant lesions occurrence and ultraviolet exposure. In contrast, the head and neck regions typically contained actinic keratosis lesions, while the trunk and extremities regions typically were sites for Bowen's disease, which is consistent with a previous report8. However, the most common site was the facial region for both actinic keratosis and Bowen's disease (97.04% in actinic keratosis and 36.22% in Bowen's disease).
In this study, 204 (15.79%) of the patients had a history of previous major skin cancers. In these patients, SCC was the most common cancer for those with actinic keratosis and Bowen's disease, which is in stark contrast with the fact that BCC is the most highly observed (48.32%) malignant skin tumor at our institution1. Interestingly, Hensen et al.12 have reported that a history of previous skin cancers is an independent predictor of actinic keratosis risk. Although there are no Korean studies regarding history of previous skin cancers of patients with cutaneous premalignant lesions, several small-scale studies of patients with actinic keratosis or Bowen's disease have reported associations between these conditions and skin cancers. In previous studies, the proportion of patients who had history of previous major skin cancers ranged from 3.17% to 7.50% for actinic keratosis and from 4.44% to 8.89% for Bowen's disease13141516. As these results are higher than the national skin cancer incidence (0.16%~2.39%) in Korea2, this suggests that a history of previous skin cancers is an independent predictor of cutaneous premalignant lesions. This correlation may be explained by the shared risk factors for cutaneous premalignant lesions and skin cancers, such as ultraviolet radiation.
In the present study, most patients had single lesions, despite the average number of lesions per patient being 2.71. The average number of lesions in patients with actinic keratosis was 3.25, with 53.1% of patients having a single lesion. In contrast, a study of Caucasian subjects reported that multiple lesions were more common than single lesions17, although Korean studies have reported that 58.9%~70.0% of patients had a single lesion131418. These findings indicate that a Caucasian background is a risk factor for actinic keratosis, and this hypothesis is consistent with the higher incidence of actinic keratosis in Caucasians19. We also found that the average number of lesions in patients with Bowen's disease was 1.48, and more patients (78.21%) had a single lesion than multiple lesions (21.79%). This finding is consistent with the results of previous Korean studies, which have reported that patients with a single lesion were more common (77%~100%)13141517.
Interestingly, Flohil et al.20 have reported that the number of lesions was associated with sex, age, skin color, area of residence (high-ultraviolet radiation region), and the extent of efforts to block ultraviolet radiation exposure. Furthermore, that study also suggested that the number of lesions was significantly correlated with a history of previous major skin cancers. We also evaluated differences in age, risk of ultraviolet exposure, and history of previous skin cancers according to the number of lesions (single or multiple) and found that all differences were statistically significant. The multiple lesion group was older (71.52 years) than the single lesion group (65.82 years, p <0.001). We also compared the proportion of outdoor workers according to the number of lesions, and found that multiple lesions were significantly more common than single lesions in outdoor workers. Similarly, Naruse et al.21 have reported that the prevalence of actinic keratosis in outdoor workers (0.64%) was significantly higher than that in indoor workers (0.28%). In addition, patients with multiple lesions were more likely to have a history of previous skin cancers, compared to patients with a single lesion. Therefore, our results confirm the previous studies' conclusions that the number of lesions was significantly correlated with age, ultraviolet light exposure, and a history of previous major skin cancers.
The limitations of our study are our use of hospital-based data, which cannot be generalized, and our Busan population has a higher education level and receives more ultraviolet exposure at lower latitudes, compared to other Korean populations.
Based on our results, Korean cutaneous premalignant lesion incidence has increased steadily. Actinic keratosis was the most common lesion. Single lesions were more common than multiple lesions, and patients were typically diagnosed between the ages of 60~79 years. Possible causes for the increasing cutaneous premalignant lesion incidence include the aging population, increased ultraviolet radiation exposure, and the public's increased awareness of malignant skin tumors and cutaneous premalignant lesions. As incidence is expected to continue increasing in the future, early diagnosis and treatment of cutaneous premalignant lesions is vital to the prevention of skin cancer.




 XML Download
XML Download