

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
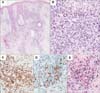
A 70-year-old woman presented with a 2-week history of facial eruption. She was treated with corticosteroid, on the basis of a diagnosis of allergic contact dermatitis, which improved her condition. However, it recurred after 1 year. She did not complain about any subjective photosensitivity or hypersensitivity to mosquito bites. Physical examination revealed multiple erythematous papulopustules with ulcers and crusts on the face, accompanied by edema on both cheeks and eyelids (Fig. 1). She was otherwise healthy, except for having had cryptogenic liver cirrhosis 7 years previously. Histopathological examination was performed on the forehead. Small to medium-sized atypical lymphocytes infiltrated around the perivascular and periadnexal spaces in the entire dermis (Fig. 2A, B). These atypical cells were positive for CD2, CD3, CD5, and T-cell intercellular antigen-1, and focally positive for CD8 (Fig. 2C, D). Some reactive cells were positive for CD4, and none of the tumor cells expressed CD56, CD20, or CD30. Additionally, the infiltrating cells were positive for Epstein-Barr virus (EBV)-encoded RNA in in situ hybridization (Fig. 2E). Laboratory tests revealed mild leukopenia (white blood cell count, 2.4×103/µl), mildly elevated liver enzyme levels (aspartate aminotransferase and alanine aminotransferase levels of 100 and 98 U/L, respectively), and elevated lactate dehydrogenase levels of 233 U/L (reference range, 100~200 U/L). The serum was positive for EBV-capsid antigen immunoglobulin (Ig) G and EBV early antigen IgG and IgM. Quantification of EBV by using real-time polymerase chain reaction (PCR) revealed 200.5 copies/µl. Ultraviolet A provocation test on the back did not provoke symptoms. PCR revealed no monoclonal T-cell receptor (TCR)-gamma gene rearrangement. Except for hepatosplenomegaly, no other evidence of systemic involvement was found. Finally, a diagnosis of hydroa vacciniforme (HV)-like eruption was concluded. At 1-year follow-up, new lesions continually arose with the application of topical corticosteroid.
HV-like eruption, or atypical HV, occurs predominantly in children and adolescents in East Asia and Latin America. It is characterized by an edematous, crusted papulovesicular eruption similar to HV1234. Unlike HV, however, it could also occur in non-sun-exposed areas, and is accompanied by fever, lymphadenopathy, or hepatosplenomegaly1234. Because HV-like lymphoma could occur in non-sun-exposed areas and is accompanied by systemic symptoms, it can be confused with HV-like eruption. However, as recent studies revealed that most lesions contain monoclonal TCR rearrangement, the World Health Organization classification system newly categorized it as one of the EBV-associated lymphoproliferative disorders of childhood in 20085. These three disease categories were related to EBV infection and predominantly occur in children and adolescents. However, HV-like eruption is occasionally observed in adults aged older than 60 years: one case was that of a 65-year-old woman with orogenital ulcer, whose symptoms were well controlled with corticosteroid and famciclovir3, whereas the other was a case of a 74-year-old man whose condition deteriorated rapidly and who died within 3 months of diagnosis4. Thus, we report a case of HV-like eruption in an older adult manifesting chronic feature. Furthermore, the disease entity needs to be clarified and the disease properties need to be investigated in future studies.

 XML Download
XML Download