

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Scabies is a contagious skin infestation caused by Sarcoptes scabiei burrowing into the epidermis. Scabies can cause clinical eruptions and intense pruritus with nocturnal exacerbation1. The presence of typical skin lesions and nocturnal pruritus enable rapid diagnosis and treatment1. Clinical eruptions, including scabietic nodules and visible skin burrows, can be the pathognomonic lesions of scabies2. However, infants and young children may present with atypical skin nodules, vesicles, and pustules that tend to be more generalized. These atypical manifestations often can be confused with seborrheic dermatitis, eczematous dermatitis, impetigo, multiple arthropod bites, and Langerhans cell histiocytosis (LCH)3. Here, we report the case of a 6-month-old infant with scabies who was misdiagnosed with LCH on the basis of histopathologic findings and clinical manifestations.
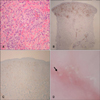
A 6-month-old girl presented with a 1-month history of erythematous to brownish papules and nodules on her trunk (Fig. 1A). The patient was initially treated with topical corticosteroid cream under a diagnosis of contact dermatitis. However, the lesions quickly spread to the patient's hands and feet, with scales and erythematous patches (Fig. 1B). Therefore, she underwent abdominal punch biopsy. Histopathologic findings showed cellular infiltrate within the upper dermis with a perivascular distribution consisting of histiocytes, lymphocytes, and eosinophils (Fig. 2A). The histiocytes in the upper dermis stained positive for CD1a and S-100 (Fig. 2B, C). Therefore, she was diagnosed with LCH on the basis of histopathologic findings and clinical manifestation. However, at that time, her mother complained of pruritus and presented with scabietic nodules on the interdigital web and periumbilical area. Dermoscopy-assisted skin scraping was performed on both the palm of the patient and periumbilical area of her mother, revealing mites and eggs in both lesions (Fig. 2D). Therefore, the patient's lesions were scabietic and not due to LCH. The patient was treated with 10% crotamiton cream and achieved complete remission after 1 week. After 1 month, the patient experienced relapse of the skin lesions on her hands and feet. Skin scraping was performed again and showed positive findings for scabies. The patient was re-treated with crotamiton 10% cream. At the last follow-up of 8 months, she was relapse free.
Infantile scabies can have diverse skin manifestations, making it difficult to correctly diagnose on the basis of clinical findings alone. The histopathologic findings of scabies are also nonspecific and are insufficient for diagnosis; they include eczematous reactions in the epidermis and perivascular area, and inflammatory cell infiltrate in the dermis4. The infiltrate usually comprises numerous histiocytes positive on CD1a and S-100 staining. Therefore, these findings can be often misdiagnosed as LCH. Meanwhile, Langerhans cell hyperplasia has been reported to be present in scabies4. The presence of scattered CD30+ cells, which appears in scabies, can aid the differential diagnosis4. In addition, using electron microscopy to assess the presence or absence of Birbeck granules, which is the hallmark of LCH, can also aid diagnosis5.
In conclusion, clinicians should be aware of confusing infantile scabies with LCH. Careful history taking including exposure to scabies and performing CD30 staining, electron microscopy, and dermoscopy will aid diagnosis.

 XML Download
XML Download