

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atopic dermatitis (AD) is a global public health concern owing to its increasing prevalence and socioeconomic burden. According to the Korea National Health & Nutrition Examination Survey, the prevalence of AD has increased from 16.6% in 1995 to 29.2% in 20051. Besides direct treatment costs, AD incurs indirect costs in the form of productivity loss, loss of employment, increased healthcare costs, and decreased health-related quality of life, ultimately incurring a large socioeconomic burden. In 2008, the Korea Asthma Allergy Foundation and the Graduate School of Public Health, Seoul National University conducted a collaborative study on the "Social Costs of Asthma" using data from the National Health Insurance Corporation. The report concludes the annual total social cost of asthma, including direct, indirect, and intangible costs, is 4.1148 trillion Korean won (KRW). In the United States, according to a systematic literature review of 418 articles on AD, the annual total national costs of AD range from United States dollar (US$) 364 million to US$3.8 billion2. However, only a few studies have assessed the economic impact of AD in Korea. Therefore, we conducted a prospective cost analysis of AD by reviewing the home accounting records of patients and evaluated the economic impact of the disease by analyzing completed questionnaires on individual annual disease burden, quality of life, and changes in medical expenses with respect to changes in health-related quality of life. To handle potential uncertainties, we compared the results with the data released by the Health Insurance Review & Assessment Board on medical costs claimed by healthcare facilities.
MATERIALS AND METHODS
Economic evaluation differs from clinical or epidemiological evaluations in that cost analysis is incorporated into the study itself. Besides clinical outcomes such as safety and efficacy, economic evaluation includes economic outcomes such as healthcare costs, healthcare utilization (i.e., hospital admission, outpatient visits, utilization of pharmacy and traditional medical clinics, etc.), costs effectiveness, cost of illness, and budget impact as well as humanistic outcomes such as quality of life, compliance, and satisfaction. The medical bills for consultations, laboratory examinations, medical procedures, hospital stays, drugs, dispensing fees, and medication storage fees make up the direct medical costs in the cost analysis (capital goods and operating expenses were not included in the present study). Direct non-medical costs comprise transportation costs and caregiver costs. Direct costs comprise direct medical costs and direct non-medical costs. Indirect costs are incurred by a loss of productivity due to sick leave, early leave, tardiness, and premature death attributable to the disease morbidity; indirect costs are usually computed according to gross domestic product per capita among the working-age population. In addition to these costs, various attempts to estimate intangible costs related to pain severity, reduced health-related quality of life, patient satisfaction, and happiness index have been made.
Study population
This study enrolled AD patients who had been referred to the dermatology departments of 3 university hospitals from June 1, 2010 to August 31, 2010. Three months of prospective data were collected from the study subjects.
Assessment of atopic dermatitis severity
AD severity was evaluated according to the eczema area and severity index (EASI). Patients with scores <16, 16~26, and >26 were categorized mild, moderate, and severe, respectively.
Economic evaluation of atopic dermatitis using home accounting records and receipts
We developed a home accounting book in order to accurately determine direct medical costs (i.e., hospital bills and pharmacy costs), direct non-medical costs (i.e., transportation costs and caregiver costs), and indirect costs. We instructed the subjects to fill out the account book and collect receipts throughout the study period. Age, sex, the number and order of siblings, and household incomes were also evaluated.
Economic evaluation of atopic dermatitis using questionnaires
We categorized the cost of illness into costs incurred by the use of hospitals, traditional Oriental medical clinics, and alternative folk medicines and compared them with the previous year's AD-related cost analysis by using questionnaires. We also analyzed the number of outpatient visits and hospital admissions during the past year to determine the level of healthcare utilization. AD severity was included in the questionnaire as well. Quality of life was assessed by utility measures using the EuroQol 5 Dimension, Korean version (EQ5D-Kor)3 and a visual analogue scale.
Economic evaluation of atopic dermatitis using electronic data interchange
We analyzed the subjects' electronic data interchange (EDI) data and compared them with the cost analysis of AD during the past year.
Perspective
We assumed the societal perspective4. In economic evaluation, the principles of equity and allocation are strongly affected by the choice of perspective such as those of the society, payer, provider, patient, or pharmacy. From the societal perspective, health economics studies include all direct medical costs, direct nonmedical cost, and indirect costs.
Data sources
Home accounting records, receipts, questionnaires, and EDI data were used as data sources for analysis.
Study period
To approximate the disease burden, data obtained from the actual 3-month study period were extrapolated to 1 year. Analysis regarding potential uncertainty was conducted.
Statistical analysis
SAS ver. 8.1 (SAS Institute, Cary, NC, USA) was used for statistical analysis. Technical analysis was performed to analyze the characteristics of the study population, direct and indirect medical cost estimates, quality of life assessment, and healthcare utilization. The relationships of healthcare costs and quality of life with disease severity were determined by ANOVA. Meanwhile, the relationship between healthcare cost and quality of life was analyzed by using a linear regression model (Kaplan-Meier curves) with a 5% significance level.
RESULTS
Economic evaluation using home accounting records
1) Characteristics of patients (or their families or guardians) who submitted home accounting records
A total of 34 home accounting records submitted to 3 hospitals (Chung-Ang University Hospital, Kyungpook National University Hospital, and Pusan National University Hospital) were included in the analysis. The mean patient age was 15±10 years. Among them, 22 patients were minors under the age of 19 years (64.7%), and 12 patients were adults (35.3%). Moreover, 18 patients were male (52.9%), and 16 were female (47.1%) (Table 1).
2) Healthcare utilization
The mean number of outpatient visits during the 3-month study period was 5.6±3.5 times. None of the subjects were admitted to hospitals during the study period. The mean number of emergency department visits for minor patients was 1 time. Among adults, 1 patient received traditional Oriental medical therapy 5 times over 3 months. The mean number of pharmacy visits during the study period was 4.8±3.4 times (Table 2).
3) Direct medical costs
The mean cost of outpatient therapy during the study was 285,317 KRW (95% confidence interval [CI], 174,810~395,825). For minor and adult patients, the mean costs were 242,310 and 364,163 KRW, respectively. For male and female patients, the mean costs were 271,519 and 300,840 KRW, respectively. The direct medical costs for outpatients were calculated by summing health insurance claims, uninsured medical expenses, and out-of-pocket payment portions of insured medical expense. Direct medical costs included consultation fees, costs of medical tests and procedures, prescription fees, dispensing fees, medication storage fees, and the costs of drugs and other dermatologic products prescribed by the hospital. The mean costs of emergency care during the 3-month study period were 36,882 KRW. The mean cost of traditional Oriental medical therapy during the study period was 42,500 KRW.
The mean pharmacy cost during the study period was 174,518 KRW (95% CI, 122,486~226,550). Direct medical costs related to pharmacy visits, which includes the costs of drugs prescribed outside the hospital, dispensing fees, medication storage fees, and the costs of other dermatological products sold in pharmacies, was calculated by summing health insurance claims, uninsured medical expenses, and out-of-pocket payment portions of the insured medical expenses.
The total direct medical costs, which were calculated by summing expenditures on outpatient therapy, drugs, and traditional Oriental medical therapy, were 457,038 KRW (Table 3).
4) Direct non-medical costs
No caregiver costs were incurred during the study period. Therefore, the mean direct non-medical costs (i.e., transportation and caregiver costs) were equivalent to the mean transportation costs: 50,038 KRW (95% CI, 28,854~71,222).
5) Costs incurred by folk medicine and expenditures on other atopic dermatitis-related products
Even though the costs of folk medicine and expenditures on other AD-related products are closely related to direct medical costs, we categorized them as a separate entity, because it was difficult to pinpoint its place in economic evaluation in terms of health economics. One minor patient spent 192,000 KRW on folk medicine AD-related AD treatment over 8 sessions during the study period.
The mean expenditure on AD-related products during the study period was 120,313 KRW (95% CI, 61,392~179,234).
6) Total direct costs
The total direct costs, which were calculated by summing the direct medical and non-medical costs, were 541,280 KRW (95% CI, 389,313~693,247). The mean direct costs for minor and adult patients were 481,205 and 643,407 KRW, respectively. Regarding sex, the mean direct costs for male and female patients were 521,117 and 575,557 KRW, respectively.
7) Indirect costs
The study population took a total of 2 days of sick leave owing to AD during the 3-month study period, both by minors. No tardiness due to AD was reported. In minors, the mean number days of early leave due to AD was 4±2 days.
For the families or guardians of AD patients, the mean number of days of work absence to assist patients was 4.5±4.9 days. The mean number of days of early leave taken by the families or guardians of AD patients was 3±2.6 days.
Economic evaluation using questionnaires
1) Cost of illness associated with atopic dermatitis in the past year
The cost of illness associated with the hospital treatment of AD in the past year was 100,000~500,000, 500,000~1,000,000, 1,000,000~5,000,000, and >10,000,000 KRW in 22%, 15%, 53%, and 3% of patients, respectively. The cost of illness associated with traditional Oriental medical therapy in the past year was 1,000,000~5,000,000 KRW in 13% of patients; 66% answered that they did not utilize traditional Oriental medical clinics.
The cost of illness related to alternative therapies such as folk medicine and self-remedies in the past year was <10,000, 100,000~500,000, 500,000~1,000,000, and 1,000,000~5,000,000 KRW in 9%, 22%, 9%, and 16%, respectively; 32% of patients replied that they did not resort to folk medicine or other alternative therapies.
The costs of illness due to expenditures on non-medical measures such as special diets or residential environment modifications during the past year were 100,000~500,000, 500,000~1,000,000, 1,000,000~5,000,000, and >10,000,000 KRW in 32%, 25%, 25%, and 3% of patients, respectively.
Economic evaluation according to home accounting records and questionnaires
1) Impact of disease severity on medical costs
The mean direct medical cost during the study period was 457,038 KRW. When disease severity according to the EASI was taken into account, the mean direct medical costs for mild, moderate, and severe AD patients were 282,850, 485,732, and 668,682 KRW, respectively. Disease severity was associated with higher direct medical costs, but this tendency was not statistically significant (p=0.082) (Table 4).
2) Impact of disease severity on utility measures
The mean EQ5D-Kor score was 0.7±0.2. When classified by severity according to the EASI, the mean EQ5D-Kor scores for mild, moderate, and severe AD patients were 0.8, 0.7, and 0.1, respectively. There was a significant relationship between utility measures and disease severity (p=0.0057; Table 5).
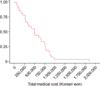
3) Impact of quality of life on total medical costs
Quality of life measured by the EQ5D-Kor was significantly inversely associated with total medical costs (p<0.001; Fig. 1).
Economic evaluation of atopic dermatitis using the electronic data interchange
The estimated mean cost of outpatient care in the preceding year (2009) according to the EDI was 1,299,830 KRW (95% CI, 339,388~2,260,273). The estimated mean costs of outpatient care for minor and adult patients were 955,223 and 1,816,742 KRW, respectively. Those for male and female patients were 1,113,855 and 1,423,814 KRW, respectively (Table 6).
Estimated cost of illness according to extrapolated data to adjust for uncertainties
Direct costs, expenditures on other AD-related products, and indirect costs were computed with the use of home accounting records and receipts during the 3-month study period. These costs were designated as 'cost inventory.' The direct cost per patient was 541,280 KRW (95% CI, 389,313.1~693,247.1), and expenditures on other AD-related products per patient were 120,313 KRW (95% CI, 61,392.3~179,234.9). We extrapolated these data to determine an annual direct cost of 2,646,372 KRW, which includes expenditures on other AD-related products. Non-attendance at school, tardiness, and early leave due to illness in minor patients were excluded from the cost calculation.
In the adult working-age population, indirect costs were calculated using the following data: mean of 4.5 days of non-attendance at work, 3 days of early leave (converted to 1.5 days of non-attendance at work), and 2010 gross national product per capita, which was estimated at US$20,000; currency conversion was performed according to foreign exchange rates on of December 30, 2010 (1 USD=1,146 KRW). The estimated indirect costs were 1,507,068 KRW. Thus, the annual cost of illness of AD, estimated by summing direct and indirect costs, was 4,153,440 KRW.
DISCUSSION
Most previous studies on AD have focused on epidemiological aspects or technical efficiency such as cost-effectiveness analyses of different medications5. Meanwhile, very few studies have addressed the cost of illness incorporating distributive efficiency and equity; in particular, such studies are hardly ever conducted in Korea.
The present study employed diverse data collection methods such as home accounting records, questionnaires, and prospective and retrospective collection of EDI in order to evaluate the economic impacts of AD. All methods were thoroughly discussed and agreed upon by multidisciplinary professional panels beforehand. Preplanned prospective economic evaluation using home accounting records and receipts is a highly valid and accurate method for cost analysis; it enables the accurate determination of healthcare utilization and medical costs including uninsured medical expenses, out-of-pocket payment portions of insured medical expenses, expenditures on other AD-related products, transportation costs, caregiver costs, and indirect costs. However, the short study period, seasonal factors, regional factors, and limitations related to large university hospitals are potential sources of uncertainty. In addition, as all patients were enrolled from university hospitals, it is possible that the cost of illness may have been overestimated.
Regarding the cost of illness calculated in this study, the direct cost of AD per patient during the 3-month study period was 541,280 KRW, and expenditures on other AD related products were 120,313 KRW. We extrapolated the data to determine the annual direct cost (i.e., including expenditures on other AD-related products) per patient of 2,646,372 KRW. We assumed the gross national product per capita of Korean in 2010 to be US$20,000 and estimated the annual indirect costs of AD to be 1,507,068 KRW. The annual cost of illness of AD, which was calculated by summing direct and indirect costs, was estimated to be 4,153,440 KRW.
Fig. 1 determined in the present study is higher than the annual average cost determined in a similar study conducted in Italy in 2006 that evaluated the economic impact of AD in children by using questionnaires filled out by the families or guardians of 33 AD patients (US$1,540 or ~1,800,000 KRW)6. In that study, the main expenses were related to moisturizing therapies and private specialist consultations. Given the time elapsed since that study was conducted as well as increased disease prevalence, inflation, and the fact that that study relied on retrospective data collection using questionnaires to gather information solely on direct medical costs, the results are comparable to those of the present study.
The estimated annual direct cost of AD per patient according to data extrapolated from the home accounting records was 2,646,372 KRW. To adjust for uncertainties, we double-checked the data against the questionnaire answers, confirming the results. The costs of illness associated with hospital treatments in the preceding year were 100,000~500,000, 500,000~1,000,000, 1,000,000~5,000,000, and >10,000,000 KRW in 22%, 15%, 53%, and 3% of patients, respectively.
Data from the EDI were also reviewed to adjust for uncertainties. According to the EDI, the mean cost of outpatient care was 1,299,830 KRW. Considering the EDI cannot provide information about the costs of drugs prescribed outside the hospital, dispensing fees, expenses on goods and services purchased from other healthcare institutions, costs of traditional Oriental medical care, expenses on other AD-related products, transportation costs, caregiver costs, or indirect costs, costs derived from the home accounting records appear valid.
Our home accounting data have some potential limitations including the short time span, regional factors, large university hospital-centered analysis, and limited reliability of the questionnaires. In addition, the data from the EDI have some limitations; in particular, expenditures related to the utilization of other medical institutions or pharmacies outside the hospital were unavailable.
A study conducted in the Netherlands in 2002 made an international comparison of the cost of AD. The total mean healthcare costs per patient in the Netherlands7 and Germany8,9 were US$71 (81,579 KRW) and US$2,559 (2,940,291 KRW), respectively. The authors suggest the variation may be due to differences in study populations including disease severity and cost components. As the present study was centered on large university hospitals, further studies are require to calculate the healthcare costs at the primary care level.
In the present study, the mean direct medical costs per patient were 457,038 KRW. When classified by severity according to the EASI, the mean direct medical costs for mild, moderate, and severe AD were 282,850, 485,732, and 668,682 KRW, respectively. Direct medical costs appeared to increase in association with increasing disease severity, although this trend was not statistically significant. The mean total direct costs (i.e., direct medical costs+direct non-medical costs) were 541,280 KRW. According to EASI disease severity, the mean total direct costs for mild, moderate, and severe AD were 521,177, 619,263, and 769,682 KRW, respectively. Again, total direct costs appeared to increase with increasing disease severity, although the trend was not statistically significant. The lack of statistical significance of these trends may be attributable to the small size of the study population. In particular, the study population included very few severe AD patients. In the 2006 Italian study, patients with moderate to severe disease severity had higher healthcare costs than those with mild disease severity; however, there was no significant difference in healthcare costs between patients with moderate and severe disease activity.
Even the present results have limited generalizability. If we assume the Korean population in 2010 to be 48,200,000, the prevalence of AD to be 29.2%, and that 10% of patients share healthcare utilization patterns similar to the present study population, the annual total social cost of AD in Korea is estimated to be ~5.8 trillion KRW. If we assume 5% of patients have healthcare utilization patterns similar to those in the present study, the total social cost is estimated to be ~2.9 trillion KRW. Even with a meager assumption of 3% of patients with similar healthcare utilization patterns, the total social cost of AD would be ~1.7 trillion KRW. On the basis of these figures, we can assume the direct medical costs of AD in Korea to be approximately 1 trillion KRW per year not including indirect costs.
The Health Insurance Review & Assessment Service (HIRA) relays the assessment results regarding medical service costs (including traditional Oriental medicine), laboratory test expenses, hospital admission costs, and medication costs of AD to healthcare providers. The HIRA data are very important, as the HIRA handles diverse patient information on a national level. In the present study, the estimated mean annual cost of outpatient care according to the EDI was 1,299,830 KRW, which is approximately one-third of the annual cost of illness of AD (4,153,440 KRW). According to the HIRA data, the total hospital and medical claims with AD listed as the primary diagnosis amounted to ~30 billion KRW in 2012. Using the extrapolation technique based on this figure, the total cost of illness of AD is estimated at 1 trillion KRW.
However, according to 2011 Acta report "Prevalence and Risk Factors for Atopic Dermatitis: A Cross-sectional Study of 6,453 Korean Preschool Children," the prevalence of AD according to the questionnaire results was 19.1% while the prevalence of physician-diagnosed AD was 9.2%. If we apply such a discrepancy to the present results, the cost of illness of AD is reduced by approximately one third; therefore, our estimates definitely have limitations and uncertainties10.
Regarding other countries, the prevalence of AD in the United Kingdom in 2003 was 11.5%, and the corresponding annual cost of illness was estimated at £465 million (~8 trillion KRW). In the United States, the disease prevalence and annual cost of AD in 2002 were estimated to be 15% to 30% and US$0.9~3.8 billion (1~4.3 trillion KRW)11, respectively. Findings from other countries suggest the global burden of AD will continue to increase steadily.
The major limitation of the present study is that we could not access the information on patients' health insurance data related to AD treatment and therefore had to rely solely on data provided by healthcare institutions and patients. Another limitation is the potential uncertainties due to the extrapolation techniques employed. Finally, the apparent lack of statistically significant relationships among disease severity, quality of life, and healthcare costs because of the small sample size is another limitation.
The present study employed a novel approach to evaluate the economic impact of AD with the specialized use of home accounting records and receipts. We also adopted various performance evaluation indices such as utility measures and disease severity to aid economic evaluation and performed analyses on healthcare utilization, indirect costs, and time spent on treatment in addition to normal cost analysis and cost of illness. In this regard, our economic evaluation is robust and of great value.
Nevertheless, further studies are required to overcome the lack of epidemiological analyses on conditions commonly associated with AD, such as asthma, allergic rhinitis, sleep disturbance, family stress, and psychosocial morbidity. In addition, further studies are recommended to overcome the lack of information regarding the use of AD medications and analyses on the cost-effectiveness of different medications.
In conclusion, a long-term large prospective study evaluating the economic impact of AD is warranted, and the National Health Insurance Corporation and Health Insurance Review and Assessment Service data should be made available to help guide efficient and equitable treatment and preventive measures.





 XML Download
XML Download