

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vitamin D insufficiency is an increasingly recognized problem among the general population, and has been largely attributed to dietary, lifestyle, and behavioral changes1. Although its musculoskeletal consequences are well established, a new hypothesis has linked atopic dermatitis (AD) to lower vitamin D levels2,3. Vitamin D has several effects on the skin that can enhance keratinocyte differentiation, increase wound healing, decrease inflammation, and induce cathelicidin (LL-37) production4,5, and these effects might be relevant in the primary prevention of AD6. LL-37 deficiency in the skin, in particular, has a known association with AD6. Recently, several studies have investigated the serum vitamin D levels of AD patients, and the correlation between serum vitamin D level and AD severity7,8,9,10; however, the results have been conflicting. Therefore, the aims of the current study are to investigate vitamin D status and the relations between serum 25-hydroxyvitamin D (25(OH)D3) level, AD severity (SCORAD score), serum LL-37 level, and body mass index (BMI) in Korean AD patients, and to explore whether these associations differ between adults (≥18 years old) and children (<18 years old).
MATERIALS AND METHODS
Subjects
Seventy-two Korean patients with AD, including 39 adults (age range, 18~51 years) and 33 children (age range, 12 months~16 years) participated in this study. The diagnosis was based on the classification of Hanifin and Rajka. The control group consisted of 140 healthy, age- and sexmatched subjects, including 70 adults and 70 children. All patients and control subjects were Koreans with phototype IV or V skin according to the Fitzpatrick classification. The study was performed from December 2012 to February 2013 to avoid seasonal variations in vitamin D levels. The demographic characteristics of the study population are shown in Table 1. None of the patients received oral or topical corticosteroids, calcineurin inhibitors, or systemic immunosuppressives for at least 4 weeks before enrollment. In addition, subjects were excluded from the study if they had received oral vitamin D or any medication known to interact with calcium in the previous 6 months. Approval for this study was obtained from the institutional review board of Eulji General Hospital (IRB No. 12-61).
Data collection
The same physician evaluated the severity of AD in all patients by using the SCORAD index. Eczema was scored in each patient as mild (<25), moderate (25~50), or severe (>50), as defined in previous studies11. Levels of 25(OH)D3 were analyzed with a chemiluminescent method (LIAISON 25-OH Vitamin D Total; DiaSorin, Saluggia, Italy). Values were used as a continuous variable and vitamin D amounts were also categorized, in a descriptive analysis, as follows: sufficient, ≥30 ng/ml; insufficient, 21~29 ng/ml; and deficient, ≤20 ng/ml. Cathelicidin expression was determined by using a human LL-37 ELISA kit (Hycult Biotech, Uden, the Netherlands).
Statistical analysis
Comparisons between the healthy control group and the AD group were made by using independent t-tests for vitamin D levels. Correlations among variables were investigated with the Pearson's correlation coefficient. Among groups presenting different AD severities as determined with the SCORAD index, a comparison of vitamin D levels was performed with ANOVA. p-values ≤ 0.05 were considered statistically significant. A commercially available software was used for data analysis (SPSS 14.0; SPSS Inc., Chicago, IL, USA).
RESULTS
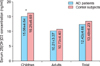
Serum 25(OH)D3 levels, representing systemic vitamin D3 status, were significantly reduced in children with AD (15.06±4.64 ng/ml) compared with the normal children in the control group (16.25±6.60 ng/ml) (p=0.036). Serum 25(OH)D3 levels were not statistically different (p>0.05) between the 72 patients with AD (12.43±4.66 ng/ml) and the 140 control subjects (13.49±6.23 ng/ml), or between adults with AD (10.21±3.37 ng/ml) and the normal adult controls (10.73±4.40 ng/ml) (Fig. 1). Levels of 25(OH)D3 in AD patients and control subjects were considered deficient in 65 of 72 (90%) and 116 of 140 (83%) subjects, respectively, and were insufficient in 7 of 72 (10%) and 23 of 140 (16%) subjects. All adults with AD (39 of 39, 100%) and 26 of 33 children with AD (78.8%) showed deficient 25(OH)D3 levels. Only one child in the control group had a sufficient 25(OH)D3 level. On SCORAD examination, 1 (1.4%) patient had mild AD, 36 (50%) patients had moderate AD, and 36 (48.6%) patients had severe AD. Differences in serum vitamin D levels among the different eczema severity groups were not statistically significant (p>0.05). Fig. 2 shows the correlations between 25 (OH)D3 levels, SCORAD scores, BMI, and serum LL-37 levels in all patients with AD. Significant inverse correlations were found between BMI and vitamin D levels (r=-0.315, p=0.007), and between SCORAD scores and serum LL-37 levels (r=-0.3, p=0.011). In the control group, a significant inverse correlation between BMI and vitamin D level was found (r=-0.335, p=0.009). After subdividing the group into adults and children, only the correlation between SCORAD score and serum LL-37 levels of adult group remained significant (r=-0.359, p=0.025).
DISCUSSION
Peroni et al.9 reported a correlation between vitamin D deficiency and the severity of AD in children, which seemed to support previous epidemiological observations suggesting a possible inverse association between vitamin D nutritional intake or exposure to the sun and AD disease prevalence12. However, other studies found no association between serum vitamin D levels and the SCORAD score7,8. In accordance with these later studies, our study did not demonstrate an inverse correlation between serum 25(OH)D3 concentration and AD severity. In asthma, another representative allergic disease, several studies have indicated that low 25(OH)D3 levels are correlated with poor disease control, reduced lung function, reduced glucocorticoid response, and consequent increased steroid use13,14,15. Goleva et al.16 reported that this association was mainly significant in pediatric patients, and not in the adult asthma group. Thus, we analyzed these correlations among variables after subdividing the patients into the adults group and the children group. However, a correlation between serum 25(OH)D3 concentration and AD severity was not found in the two groups17.
Several studies in Korea have indicated a high prevalence of vitamin D deficiency in healthy Koreans17,18,19. Koreans are theoretically at an increased risk for vitamin D insufficiency because of living at high latitudes and because of their increased use of sunscreen, reduced outdoor activities, and a lack of intake of vitamin D-fortified foods17,20.
According to one investigation during winter, the prevalence of vitamin D deficiency in Koreans was >90%18. In agreement with these results, our study revealed that 90% of patients with AD and 83% of healthy controls were vitamin D deficient. The difference in serum vitamin D levels between these two groups was not statistically significant; however, in subgroup analysis, children with AD showed significantly lower serum vitamin D levels than age- and sex-matched healthy controls. Most allergies begin in childhood; thus, the significantly lower level of vitamin D observed in young AD patients might be related to the initiation of AD.
In this study, serum LL-37 was used as a vitamin D-regulated target. LL-37 is one of the most well-known antimicrobial peptides, and it acts against bacteria, viruses, and fungi6,21. Reduced expression of antimicrobial peptides may cause recurrent infections, and decreased LL-37 expression is known to be associated with AD6,21. Vitamin D enhances LL-37 production in keratinocytes because promoters of cathelicidin genes contain consensus vitamin D response elements4. Oral vitamin D3 has been shown to increase cathelicidin expression in AD lesions22. Kanda et al.10 recently reported that serum LL-37 levels correlated with 25(OH)D3 in AD patients. However, in the present study, we did not observe a positive correlation between 25(OH)D3 and serum LL-37 level in any group. We assume that these conflicting results may be because serum LL-37 is produced by multiple cell types, and a number of vitamin D-independent pathways control LL-37 production23. Of interest, a significant inverse correlation was found between the SCORAD score and serum LL-37 level in all AD patients and in the adult AD subgroup. This finding is in contrast with the results of Leung et al.24, who reported that serum LL-37 levels show a positive correlation with eczema severity in children, suggesting that circulating LL-37 might be a biomarker for eczema severity. The basis for the differences between these studies remains unclear; however, our results suggest that LL-37 production decreases in proportion to AD severity.
As previously reported25,26, we observed a significant negative correlation between BMI and serum 25(OH)D3 concentration. One reason proposed for this relation has been the presumed lesser physical activity and, therefore, reduced sun exposure of overweight and obese persons27. Another possible explanation is that body fat may act as a sink for vitamin D, which could be deposited in an almost irreversible manner, and is not bioavailable28.
In conclusion, we observed that most participants in both the AD and control groups were vitamin D deficient. Vitamin D levels were lower in children with AD than in controls; however, the same relation was not observed in adults with AD. There were statistically significant correlations between BMI and serum 25(OH)D3 concentration in all participants, and between the SCORAD score and serum LL-37 level in all AD patients and in the adult AD subgroup; however, we were unable to detect an inverse correlation between serum vitamin D level and the SCORAD score.
Recently, the beneficial effect of oral supplementation with vitamin D has been reported in several studies8,29,30. However, additional investigations on the association between vitamin D and AD, as well as on the effects of vitamin D supplementation are needed in a larger study population before vitamin D can be recommended as a treatment option for AD.


 XML Download
XML Download