

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The scalp is a relatively common site of cutaneous metastasis, usually presenting as a single or multiple firm scalp nodules1,2. Alopecia neoplastica is a well-recognized but rare presentation that, manifests as a single or multiple areas of cicatricial alopecia. Herein we report a rare case of alopecia neoplastica due to metastatic gastric adenocarcinoma and review the relavant literature.
CASE REPORT
A 33-year-old woman was referred for a subcutaneous nodule on the surface of an erythematous-, hairless patch on the frontal scalp observed 3 months previously, to rule out metastasis from her known gastric adenocarcinoma diagnosed in January 2008. She had undergone total gastrectomy for the gastric carcinoma diagnosed in May 2007; she subsequently underwent 6 cycles of chemotherapy and total abdominal hysterectomy with bilateral salphingo-oophorectomy after being diagnosed with metastatic adenocarcinoma (Krukenberg cancer) in November 2007.
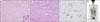
Examination revealed no abnormalities besides a scalp lesion exhibiting a hard, movable, non-tender subcutaneous nodule covered with a slightly erythematous alopecic patch (Fig. 1). The patient did not report any previous dermatological diseases at the site of alopecia. Routine laboratory test results including full blood count, liver function, renal function, electrolytes, chest radiography and electrocardiogram were all normal. Histopathological examination of the scalp lesion showed decreased hair follicle cells, as well as metastatic adenocarcinoma cells interspersed between collagen bundles and around hair follicles (Fig. 2A, B). Similar to the original gastric cancer, tumor cells stained positively for tumor marker MSH-2, the DNA mismatch repair protein (Fig. 2C). The total gastrectomy specimen showed signet ring cells (Fig. 3A) and poorly differentiated adenocarcinoma cells (Fig. 3B) which stained positive for MSH-2 (Fig. 3C). MSH-2 is a marker of a major mismatch repair gene, MSH-2. Polymorphisms in the MSH-2 gene were recently suggested to modulate an individual's susceptibility to gastric cancer3. Although there were no signet ring cells, the scalp specimen showed scattered, poorly differentiated, MSH-2-positive carcinoma cells. Whole body positron emission tomography (PET) scanning showed no other abnormal uptake than in the stomach (Fig. 3D). Following colonoscopy with biopsy also revealed no malignancy. PET scanning performed after total abdominal hysterectomy with bilateral salphingo-oophorectomy in November 2007 revealed no remaining malignancy. Therefore, we concluded the scalp metastasis originated from the gastric cancer. Cutaneous metastasis usually exhibits features consistent with the underlying malignancy. However, the metastasis may exhibit less differentiation and be more anaplastic. Therefore, we can infer that atrophy of the hair follicles and gastric cancer invaded the collagenous stroma, influencing the development of alopecia. On the basis of both clinical and histopathological findings, the patient was diagnosed with alopecia neoplastica due to gastric adenocarcinoma. Despite performing the cancer chemotherapy, no hair regrowth was observed.
DISCUSSION
The overall incidence of cutaneous metastasis from visceral carcinomas ranges from 0.7%~9%4. The scalp is a relatively common site of cutaneous metastasis. Brownstein and Helwig1 report that the scalp is the site of 4% of all skin metastases, usually presenting as single or multiple nodules5,6,7,8. The most frequent manifestation of scalp metastasis is the occurrence of single or multiple non-tender nodules that usually appear suddenly and grow rapidly9,10. Alopecia neoplastica is a well-recognized but rarer manifestation that presents as a single or multiple areas of cicatricial alopecia. To our knowledge, 29 patients with alopecia neoplastica including the one described herein have been reported in the literature (Table 1)1,8,11,12,13,14,15,16. A review of these cases revealed that alopecia neoplastica is usually a presentation of breast cancer metastasis, and other primary sites are extremely rare. Yuen et al.15 reported a case in which the primary tumor was a placental trophoblastic tumor. Furthermore, metastases from colon and cervical cancer have also been reported. Kohno et al.14 and Kim et al.8, each of them reported 2 cases of alopecia neoplastica due to metastasis from gastric carcinoma. Meanwhile, only 3 cases of alopecia neoplastica due to gastric carcinoma, including this case, have been reported, among them 2 cases were alopecia neoplastica due to signet ring cell-type gastric carcinoma. Because of the small number of cases, it remains unclear if the metastatic potential of signet ring cell-type gastric carcinoma is greater to the skin or scalp. However, a recent study about the characteristics of gastric adenocarcinoma shows that signet ring-cell gastric cancers are more differentiated and less aggressive than non-signet ring-cell gastric adenocarcinoma17. Nevertheless, the mechanism of alopecia neoplastica is uncertain. Histopathological examination of the scalp in alopecia neoplastica demonstrates metastatic carcinoma cells in a dense collagenous stroma, which is observed in the dermis and subcutaneous tissue with a loss of pilosebaceous units18. However, most malignant tumors evoke a stromal response, which is usually in the form of fibroplasia. Moreover, it is unclear if fibrosis or the release of cytokines from tumor cells leads to the disappearance of hair follicles. It is difficult to explain the complete disappearance of pilosebaceous units, but a loss of hair follicles may be the result of fibrosis; Cohen et al.16 consider this to be the major mechanism. In particular, lobular breast carcinoma, which accounts for 10% of invasive breast carcinomas, usually elicits reactive fibrosis, which leads to cicatricial alopecia. Factors independent of fibrosis, such as tumor invasion of the hair sheaths, may play a role in the development of alopecia, because hair may be regrown in alopecic areas after effective cancer treatment19,20. In the present case, metastatic adenocarcinoma cells were interspersed between collagen bundles and around hair follicles. Immunohistochemical staining was positive, which explains tumor cell infiltration around hair follicles. These findings corroborate the hypothesis that dermal infiltration of cancer cells causes the disappearance of hair follicles. Furthermore, infiltration of metastatic cancer cells into the dermis and subcutaneous tissue may put pressure on and destroy hair follicles, eventually causing alopecia.
In summary, we report a case of alopecia neoplastica due to gastric adenocarcinoma, which is a well-recognized but extremely rare manifestation of cancer metastasis to the skin. This report may be helpful for understanding the mechanism of alopecia neoplastica. Regardless, further study is needed to elucidate the specific pathologic mechanism of this disease.



 XML Download
XML Download