

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Psoriatic arthritis (PsA) is a chronic, inflammatory arthropathy associated with psoriasis that affects the distal joints of the hands (distal interphalangeal), feet (metatarsophalangeal), and the spine1. PsA can affect up to 30% of persons with psoriasis, usually 5~12 years after the start of the skin involvement. In the United States and Turkey, dermatologists manage most of the psoriasis cases; therefore, these dermatologists are in an ideal position to perform early screening of PsA in patients2. The exact prevalence of PsA is unknown, and its estimation has been difficult, partly owing to a lack of widely accepted classification criteria3. The disease may not be readily diagnosed, especially during its initial presentation before the typical joint or skin involvement is evident2,3. Initially, most patients might disregard their joint symptoms as an old sport injury or simply an isolated mechanical derangement, such as a cartilage tear. Patients do not necessarily complain of all symptoms related to PsA to their primary care providers, dermatologists, or rheumatologists. However, early diagnosis is important to prevent irreversible and long-term damage to the joints4.
To help dermatologists screen psoriatic patients with symptoms of inflammatory arthritis, Harvard University, Brigham and Women's Hospital developed the psoriatic arthritis screening and evaluation (PASE) questionnaire in English5,6, a self-administered 15-item questionnaire. A pilot study in 190 persons with psoriasis demonstrated that the English-language PASE was able to distinguish PsA from non-PsA patients, with 76% sensitivity and 76% specificity6. Three other screening tools have been developed to screen for PsA: the Psoriatic Arthritis Questionnaire by Peloso7, the Toronto Psoriatic Arthritis Screening Tool by Gladman8, and the Psoriasis Epidemiology Project (personal communication)6.
The aim of this study was to evaluate the PASE questionnaire in the Turkish language to identify patients with PsA in dermatology clinics.
MATERIALS AND METHODS
Study population
Adults between the ages of 18 and 85 years with a diagnosis of psoriasis and who were able to read and understand Turkish were eligible for the study. We surveyed 122 consecutive psoriasis patients who presented to our dedicated psoriasis clinic. In this study, we excluded five PsA patients who were already receiving systemic treatment and four patients with missing scores who could not be reached. We also excluded patients with a concomitant diagnosis of other arthritis such as osteoarthritis, gout, or rheumatoid arthritis. All psoriasis patients had psoriasis vulgaris. The gold standard for diagnosis of psoriasis was based on the clinical evaluation by a dermatologist (Burhan Engin) and the diagnosis of PsA was based on the clinical evaluation by a rheumatologist (Gülen Hatemi) after patients completed the questionnaire. Specifically, the clinical diagnosis of PsA was determined by using the Moll and Wright criteria, which includes the presence of inflammatory arthritis (peripheral arthritis such as sacroiliitis or spondylitis) and psoriasis, and the absence of rheumatoid factor9. We asked for a radiograph when needed. All of the PsA cases were new, and the patients had not received therapy yet. Patients who had received treatment with systemic agents such as methotrexate, cyclosporine A, biologic agents, and other systemic drugs during the last 6 months were excluded from the study. Patients were recruited at the psoriasis outpatient clinic of the Department of Dermatology, Cerrahpaşa Medical Faculty, İstanbul University. After completing the questionnaire, the patients were sent to the rheumatology clinic for examination for PsA.
Questionnaire
Backward-forward translation of the questionnaire was made, and no meaningful differences were found. The Turkish PASE was designed for use in a busy clinical practice for screening purposes. The Turkish PASE was created by using plain language for legibility and for reaching as wide an adult audience as possible. The Turkish PASE questionnaire, consisting of 15 items, was divided into two subscales: a seven-item symptoms scale and an eight-item functions scale. Standardized response choices consisted of five categories relating to agreement (strongly agree, agree, no idea, disagree, and strongly disagree). A response of "strongly disagree" was scored with one point, "disagree" with two points, "no idea" with three points, "agree" with four points, and "strongly agree" with five points.
The scale chosen and the assignment of scores ensured that patients with a higher likelihood of having PsA would score numerically higher than non-PsA patients. The total questionnaire score was calculated by summing the responses to all 15 questions, and scores for functions and symptoms were calculated by summing the responses to the corresponding questions. The total score ranged from a minimum of 15 points to a maximum of 75 points. The maximum symptom score was 35, and the maximum function score was 40. Most individuals completed the Turkish PASE within 5 min and scoring took no more than 1 min to complete. The Turkish PASE inquires about the participants' current health.
We changed one of the questions related to socioeconomic differences between the United States and Turkey (Question 11 of the original PASE: I have had trouble getting into or out of a car. Turkish PASE: I have had trouble getting into a bus or a car.).
The rheumatologist and the dermatologist were unaware of the patients' scores during the examination of patients, and all data were calculated at the end of the research.
Analysis
The goal of this analysis was to determine the validity and reliability of the Turkish version of the PASE questionnaire. We used the Spearman correlation coefficient for determining the test-retest reliability. We also used receiver operator curves to select the best cutoff point for the total PASE score to predict PsA.
Besides these statistical methods, we calculated the sensitivity and specificity by evaluating the answers "agree" and "strongly agree" as positive and "disagree" and "strongly disagree" as negative. We excluded answers of "no idea" in this tool.
We collected the psoriasis area and sensitivity index (PASI) scores of psoriasis patients. We compared the PASI scores with the PASE scores in all patients, and the PASI scores between the PsA (p=0.899) and non-PsA (p=0.941) patients (Fig. 1). PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA) was used for data analysis.
RESULTS
Results of the 113 patients' Turkish PASE scores
We collected the PASI scores of all patients. In the 113 patients, the PASI scores ranged from 0.3 to 28.2 (mean±standard deviation; 5.3±5.03). Within this group, the mean PASI score of non-PsA patients was 5.33 and that of PsA patients was 5.17.
Validity
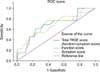
In Turkish PASE, the scores of PsA patients significantly differed from the scores of non-PsA patients (Table 1). In the PsA group, the median total score was significantly higher (49) than that of the non-PsA group (35). All arthritis patients had PsA. The total PASE scores ranged from 15 to 64 in this study, and the total PASE score of 44 was determined to be the optimal cutoff point for distinguishing PsA from non-PsA participants. At this cutoff point, the sensitivity was 62% (95% confidence interval [CI], 32%~86%) and the specificity was 76% (95% CI, 66%~84%); that is, a PASE total score of ≥44 would classify 62% of the participants as having PsA (Fig. 2). The Turkish PASE questionnaire missed 5 of the 13 PsA patients because their total PASE score was below 44. Among the 100 psoriasis patients without PsA, 23 were positive according to the results of the questionnaire.
For further analysis of each question, we counted the responses according to symptoms (positive for "agree" and "strongly agree," negative for "disagree" and "strongly disagree") and the sensitivity ranged from 23% (third question of the functions subscale) to 77% (second question of the symptoms subscale, first and fifth questions of the functions subscale) and the specificity ranged from 51% (second question of the symptoms subscale) to 87% (fourth question of the functions subscale) (Table 2).
Reliability
We administered Turkish PASE twice (>2 weeks apart) to 9 psoriasis patients and 15 healthy medical students. Spearman's correlation coefficients were used to assess the test-retest reliability of each PASE question. Thirteen of the 15 questions correlated between the two periods (p<0.05; Table 3). The p-value ranged from 0.0059 (third question of the symptoms subscale) to 1 (fifth question of the symptoms subscale and eighth question of the functions subscale).
DISCUSSION
This study shows that the Turkish version of the PASE questionnaire is not an adequate tool for identifying PsA patients in a dermatology clinic. Although it has a relatively high specificity for distinguishing PsA patients, the sensitivity for identifying PsA patients is lower than that of the original PASE questionnaire. Nevertheless, Turkish PASE has good test-retest reliability.
The cultural differences between Turkish and American patients could be one of the factors responsible for this difference. We practiced translated questionnaires at Cerrahpaşa Medical Faculty before and their responses on Turkish language were also different from the questionnaire of the original language.
Another factor could be the shortcoming of this questionnaire in detecting patients who are not active when the questionnaire was applied. The Turkish PASE questionnaire missed 5 of the 13 PsA patients because their total PASE score was below the cutoff of 44. Of these five PsA patients, four were not active during the examination by the rheumatologist after the completion of the questionnaire. The mean score of these four patients was 27, whereas the mean score of the PsA group was 49 and that of the non-PsA group was 35 (Table 1).
In this research, we collected the PASI scores of all patients. We compared the PASI scores with the PASE scores in all patients, and the PASI scores between patients with and those without arthritis. No relation was found between the PASI scores of patients with and those without arthritis, as well as between the PASI and PASE scores of individual patients (Fig. 1).
The Turkish PASE questionnaire has some limitations. Some of the scores were low because the PsA symptoms were not active during the completion of the questionnaire by the patients. In this questionnaire, few data could change the sensitivity of the research. Another limitation of this questionnaire was that the responses could differ among patients with respect to their symptoms, and this could change the sensitivity of the results.
Although the Turkish version of the PASE questionnaire is not an adequate tool for screening patients for PsA in a dermatology clinic, its relatively high specificity makes it a candidate tool for screening PsA in psoriasis patients for inclusion in trials. PsA causes irreversible joint damage, and psoriasis skin lesions usually precede the onset of PsA in up to 30% of patients2. Referring all psoriasis patients to a rheumatologist may not be practical, especially in busy practices. Thus, dermatologists are in a critical position to identify patients with a possibility of having PsA. A noninvasive, easy-to-practice, and self-administered tool that has been validated would be appropriate to use during routine psoriasis examinations. This way, PsA screening can be done at psoriasis clinics. Further research is required to develop a new questionnaire with good sensitivity and specificity for screening Turkish patients with psoriasis for PsA.




 XML Download
XML Download