

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
Confluent and reticulated papillomatosis (CRP), a rare skin disorder of unknown etiology, is characterized by hyperkeratotic papules confluent in the central area and reticulated hyperpigmented patch in the peripheral area1. Since Gougerot and Carteud first identified CRP in 1927, this disease has been diagnosed by using clinical courses, histological findings, and treatment results. However, other diseases, such as fungal infection or other pigmentary skin diseases, were frequently misdiagnosed as CRP because of the lack of diagnostic criteria for CRP. Therefore, Davis et al.1 proposed the diagnostic criteria for CRP on the basis of a study on 39 patients, as follows: (i) clinical findings of scaly brown macules and patches, with at least some appearing reticulated and papillomatous; (ii) involvement of the upper trunk and neck; (iii) negative fungal staining of scales; (iv) no response to antifungal treatment; and (v) excellent response to minocycline. However, a few cases of CRP sparing the upper trunk have also shown the typical histopathological findings, clinical findings, and treatment responses of CRP.
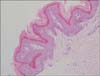
A 42-year-old Korean woman presented to our clinic with a 4-year history of asymptomatic, brownish, and reticulated skin lesions in her antecubital and axillary regions (Fig. 1A). She reported that her skin lesions had worsened in May and improved slightly in October without any specific treatment. We performed a potassium hydroxide test to rule out fungal infection. Because the test result was negative at the antecubital fossa but positive at the axilla, we began treatment with oral itraconazole and topical flutrimazole cream for 2 weeks. Despite the 2 weeks of treatment, her skin lesions persisted. We then performed an axillary skin biopsy. Histopathological evaluation revealed papillomatosis and hyperkeratosis of the epidermis, and downward growth of the epidermis between the rete ridges (Fig. 2). Periodic acid Schiff staining did not reveal any fungal organism. On the basis of these findings, we diagnosed her condition as CRP limited to the flexural areas. After 2 months of doxycycline treatment (100 mg twice a day), her skin lesions completely disappeared (Fig. 1B).
Our patient exhibited only limited lesions at the antecubital fossae and axilla, which is inconsistent with the previous diagnostic criteria for CRP1. Several cases of CRP had involved various flexural areas alone, including the axilla2,3, popliteal fossa2, or antecubital regions4. These lesions fulfilled other diagnostic criteria for CRP. Therefore the criteria related to the primary affected sites should be revised. In addition, the criteria for fungal staining and response to antifungal treatment should be modified. Occasionally, CRP and fungal infection coexist5, as in this patient, however an important diagnostic consideration is that CRP lesions cannot be improved with antifungal treatment even in the presence of a positive fungal examination. Finally, minocycline3,4 has been known as the treatment of choice for CRP; however, other antibiotics have also been efficacious3. The exact reason for the effect of antibiotics is unclear, but many dermatologists speculate that their anti-inflammatory effect may be more predominant than their anti-bacterial effect1.
As mentioned above, the previous diagnostic criteria for CRP had several limitations in cases of unusually involved location, co-infection with fungus, and use of antibiotics other than minocycline. Therefore, we propose a modified diagnostic criteria, as follows: (i) clinical findings includeing scaly brown macules and patches, with at least some appearing reticulated and papillomatous; (ii) involvement of the upper trunk, neck, or flexural areas; (iii) negative fungal staining of scales or no response to antifungal treatment; and (iv) excellent response to antibiotics.

 XML Download
XML Download