

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The differential diagnosis of bluish-gray discoloration of the skin includes benign melanocytic nevi, such as Mongolian spots, blue nevi, junctional nevi, or nevi of Ito and Ota, and malignant melanoma as well as metallic discoloration1,2. Although histopathologic findings are important for differentiating benign melanocytic nevi from malignant melanomas or metallic discoloration, a thorough history and physical examination may also provide significant information1.
Metallic discoloration is an uncommon disorder defined by the accumulation of metallic particles in the skin through the blood stream or surface application3, while metallosis refers to the deposition of metallic particles after being worn out by artificial articulation after total joint replacement4.
To the best of our knowledge, only 2 cases of titanium pigmentation have been reported in dermatologic literature5 and orthopedic literature6.
Here, we describe a case of metallic discoloration induced by titanium-aluminium alloy in a patient with a history of bilateral total knee replacements, presenting with symptoms of bluish-gray pigmentation of the right shin.
CASE REPORT
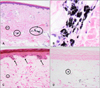
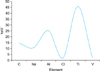
A 75-year-old woman had a large blue patch on the right shin for 3 years. She underwent a left total knee replacement 18 years ago and a right total knee replacement 14 years ago due to severe osteoarthritis of both knees. Each of the operations was carried out successfully without any serious adverse events. Eleven years after the right total knee replacement, she noticed a discoloration of her right shin, and the lesion continued to enlarge slowly over time. She was referred to a dermatology clinic where a large, well-demarcated bluish-gray patch was noted on her right shin. The surface of the skin was smooth with no palpable infiltration. For 1 year, she experienced pain when walking on the right shin. She had a 10×15 cm well-demarcated bluish-gray patch on the extensor surface of her right shin (Fig. 1). Routine laboratory tests, including complete blood count, liver function tests and urine analysis, yielded normal findings. Histopathologic findings from the skin lesion showed perivascular, fine black particles in the dermis (Fig. 2). The black particles were stained positive with both melanin and demelanin stains. Polarizing microscopy of the skin specimen revealed refractile foreign materials in the perivascular area of the dermis (Fig. 3). Further, energy-dispersive X-ray spectrophotometry revealed the presence of titanium and aluminium (Fig. 4). Metallic discoloration was diagnosed on the basis of clinical, histopathological, polarizing microscopy and energy dispersive X-ray spectrophotometer findings. The radiographs revealed loosened and dislocated tibial components of the right knee prostheses. Preoperative and intraoperative cultures were negative for bacteria. During surgical revision, marked loosening of the tibial component and wearing of polyethylene were found. Additionally, an intense black staining of a substantial amount of wear debris adjacent to the tibial components and tibial bone defect was observed (Fig. 5). The patient was treated by debridement, and the right tibial component was replaced. After the revision procedure, metallic discoloration disappeared and has not reoccurred over the past 4 years.
DISCUSSION
Metallic discoloration is caused by a deposition of metallic particles in the skin, mostly via the blood stream, external exposure or rarely, by metallosis of the prostheses. This pigment change takes place via the deposition of metal particles and induction of epidermal melanin production7. Metallic discoloration by copper7, silver8 and thallium9 has been reported in dermatologic literature.
This case presented several interesting features: (i) localized bluish-gray pigmentation mimicking the clinical picture of dermal melanocytosis caused by metallosis of an artificial joint in the knee, and (ii) the importance of considering the history of joint replacement surgery when there are bluish-gray skin lesions in an elderly patient in order to differentiate dermal melanocytosis from blue nevi or malignant melanoma.
Titanium alloy (Ti-Al6-V4) has been widely used as a material for total knee replacement surgery ever since 198510. It is composed of 90% titanium, 6% aluminium and 4% vanadium4. Metallosis of titanium alloy has frequently been reported in orthopedic literature as black staining of the periprosthetic tissue due to debris from the metallic wear and tissue reaction after knee or hip replacement surgery11.
Metallosis is usually confined to the joint capsule or around the prosthesis. Metallosis of the overlying skin is quite rare9.
To the best of our knowledge, there have been only a few cases of titanium pigmentation of the skin in the literature5,6. Seong et al.6 reported 6 cases of failed total knee replacement with titanium-induced tissue response in 5 patients. Of the 5 patients, only 1 presented symptoms with metallic discoloration. Akimoto et al.5 reported an 80-year-old woman with solid red-brown nodules and papules with scattered bluish-black macules on her right lower leg after a total lateral replacement of the right hip 6 years ago.
Histopathologically, metallosis of skin shows fine brown/black particles consistent with metallic debris throughout the dermis in the subcutaneous tissue. They are mainly phagocytosed by macrophages, but can also be seen as dispersed particles12. In addition, metallosis of periprosthetic tissue is usually composed of fibroblastic tissues, with a heavy deposition of black fragments lying extracellularly and within histiocytes and foreign-body giant cells11. It is well known that metallosis has been implicated in implant failure by causing a darkly stained proliferative soft-tissue reaction11. Unfortunately, in our case, studies to identify titanium in the affected periprosthetic tissue were not performed.
The mechanism of metallic pigmentation caused by metal-wear debris in the overlying skin remains unclear. Agins et al.11 discovered that there was no correlation between the titanium content of the tissue and the length of time that the implant had been in the body. Moran et al.13 reported 4 patients who were presented with titanium dioxide in the lungs caused by inhalation. These patients had large quantities of dark pigments in the macrophages of the peribronchial lymph nodes, liver, spleen, alveolar spaces, and around the bronchioles and blood vessels11. This suggests that macrophage-laden or free black metallic particles may spread to adjacent blood vessels and lymph nodes. In our case, the histologic appearance of the skin lesion showed black pigments predominantly in the perivascular area of the dermal and subcutaneous tissue. Further, it demonstrated a titanium and aluminium peak on the energy dispersive X-ray spectrophotometer unit attached to a transmission electron microscope. A vanadium (V) peak could not be identified because it is quickly released from tissues due to its high solubility (Fig. 4)14.
Presumably, we suggest that the periprosthetic tissue reaction of metallosis gradually spreads via lymphatic or blood vessels, and bluish-gray pigmentation subsequently develops on the overlying skin.
In summary, wear debris from a total knee joint prosthesis produced sufficient clinical symptoms, prompting the need for operative revision 14 years after implantation and 3 years after skin pigmentation on the right knee. Even though metallosis of titanium alloy is a relatively wellnown disease in orthopedic literature, metallic discoloration of the skin is quite rare, mimicking the clinical picture of blue nevi or malignant melanoma. Therefore, the possibility of metallic discoloration must be included in the differential diagnosis of bluish-gray pigmentation.



 XML Download
XML Download