

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although usually not a life-threatening condition, a skin disease can contribute to various degrees of psychosocial impairment and alter a patient's quality of life1-3. Many patients with skin disease are significantly distressed because the disease affects visible parts of the body4,5 and/or because it causes intractable symptoms such as itching or pain. Some review articles suggest that depression is one of the most common psychological co-morbidity in patients with dermatologic disorders6-8.
In general, depression is a relatively common disorder in older patients, and often occurs in the context of a physical impairment9. In a study by Watkins et al.10, the severity of depression correlated significantly with that of medical comorbity. Likewise, depression adversely influences the outcome of comorbid health disorders in the elderly11. According to a large number of studies on the psychosocial impact of neurological and medical illnesses, increased rates of depression were found to be associated with conditions such as cardiovascular disease10,12, stroke13,14, Alzheimer's disease15, and Parkinsons disease16. However, little has been reported on the association between depression and dermatologic diseases in the geriatric population. Therefore, we have conducted a survey to investigate the hypothesis that geriatric patients with dermatological disease are at an increased risk for depression in Korea. We have also sought for non-dermatologic variables that might predict depression.
MATERIALS AND METHODS
Subjects
A total of 325 patients were recruited from the Department of Dermatology at The Catholic University of Korea, St. Mary's Hospitals (Seoul, Uijeongbu, and Bucheon) from February to September 2011. Using the definition of 'elderly' by World Health Organization and United Nations (UN)17,18, patients over the age of sixty attending the department qualified for the survey.
The survey was conducted after routine dermatologic visit, and was completed by the patients themselves. For patients who did not understand portions of the questionnaire, a physician was available to answer any question.
The study design was approved by the Institutional Review Board of The Catholic University of Korea College of Medicine before the survey began. Only patients who had been instructed about the study and had granted written informed consent were enrolled.
Methods
In order to obtain a patient-based measurement of depression, the Geriatric Depression Scale (GDS) was used. The GDS was developed to assess depression in the elderly19, and it is a widely validated questionnaire that is easy to understand and quick to complete without supervision. It consists of 30 questions, each with 2 possible answers scored either 0 or 1, and gives a maximum score of 30. Scores of 0 to 9 indicate no depressive symptoms; scores from 10 to 19 indicate mild depression; and scores from 20 to 30 indicate severe depression.
In addition to the GDS, the survey questions included demographic data (age, gender, marital status, education, and family structure) as well as medical history (diagnosis, disease categories, disease duration, history of recurrence, previous treatment history, satisfaction with current treatment, concurrent disease and general health).
Statistical analysis
Absolute and relative frequencies were analyzed for all data. Constant variables, such as age, were expressed as mean values with standard deviations. The difference in the prevalence of depression between the elderly patients in our study and general population was evaluated according to Fisher's exact test. Univariate analysis was used for statistical analysis. Multiple regression analysis of variance was performed for several explanatory characteristics against the GDS score. In all cases, p<0.05 were considered significant.
RESULTS
Characteristics of participants
Of the 325 patients recruited, 313 patients had completed the survey and were included in this study. The study population consisted of 125 men and 188 women with a mean age of 69.04±6.3 years. Most were married (65.81%) and lived with the spouse (42.81%). 20.13% of patients had a university degree (Table 1).
The sampling represented a patient population with a wide variety of skin diseases. The most common were pruritus/prurigo (17.57%), herpes zoster (8.31%), fungal infection (7.99%), contact dermatitis (7.03%), psoriasis (5.43%), urticaria (4.47%), vitiligo (4.47%) and atopic dermatitis (3.17%). As a group, infectious skin diseases was the most common and was found in 22.36%. The second most frequent disease group was eczema (18.53%), followed by pruritus/prurigo and psychocutaneous disorders (17.87%), tumors and nevi (11.18%), urticaria, drug eruption, and erythema (8.31%), and papulosquamous diseases (5.43%).
The mean duration of dermatologic disease was 3.23 years (<1 month, 14.3%; 1~3 months, 13.42%; 4~6 months, 8.63%; 7~12 months, 17.57%; >12 months, 46.01%).
Psychological impact of dermatological diseases
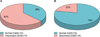
Overall, the mean GDS score was 12.35±7.13. With respect to distribution, mild (GDS 10~19) and severe (20~30) depressive symptoms were found in 143 (45.69%) and 52 (16.61%) patients, respectively, with 118 (37.70%) patients having no depressive symptoms According to a study by Lee et al.20, that investigates socioeconomic and health-behavioral risk factors of geriatric depression using the GDS, the prevalence of depression among people over the age of sixty five in an urban community was about 22.2% in Korea, and this data was used for baseline comparison. The prevalence of depression in geriatric people with skin disorder, 62.3%, was greater than that reported of the general elderly population in Korea (p<0.0001) (Fig. 1).
Association between demographic factors and Geriatric Depression Scale scores
Univariate analysis showed a significant association between education level and individual GDS score. In particular, the patients with high school (p=0.0441) and university diploma (p=0.0004) had significantly lower GDS scores than those patients without high school diploma (Fig. 2A).
Patients who lived alone (11.82%) had the highest mean GDS score of 14.31±7.71 when compared to those living with a spouse (26.52%, GDS 12.13±7.17); living with descendent(s) (10.86%, 12.12±7.07); and living with a spouse and descendent(s) (12.14%, 11.78±6.69). However, this difference was not statistically significant. Gender, age, and marital status were not found to be associated with GDS score (Table 1).
Multiple regression analysis did not reveal any independent correlates to the GDS score.
Association between disease characteristics and Geriatric Depression Scale scores
Under univariate analysis, the relationship between the GDS and physical fitness was statistically significant. Patients who reported 'very poor' fitness were 36.43 times more likely to be depressed than those who reported 'very good' physical health (p<0.0001) (Fig. 2B). Patients who suffered from concurrent disease including hypertension, liver disease, chronic kidney disease and cancer were significantly more depressed (p=0.0003). Previous medical diagnosis, disease duration, recurrence of illness, previous treatment history, and treatment outcomes were not significant risk factors for depression (Table 2). Furthermore, multiple regression analysis did not identify any clinical factors that independently related to the GDS.
DISCUSSION
Psoriasis and vitiligo have long been recognized to be associated with potentially adverse effects on mental health. In addition, there has been studies that evaluated psychological influences of dematologic diseases on the issue of quality of life, measured with the Dermatology Life Quality Index21-23. The differences in study methodology (e.g., differences in patient recruitment and population characteristics) on depression and skin disease make a direct comparison among these studies difficult, but patients with psoriasis were found to be at an increased risk of depression. Kurd et al.24 reported that the adjusted hazard ratio for receiving a diagnosis of depression in patients with psoriasis, when compared with the respective control population, was 1.31 (95% confidence interval, 1.37~1.41).
To our knowledge, the analysis of a specific relationship between dermatological diseases and depression in the elderly population has not been previously reported. In our study, mild to severe depression was observed in 62.3% of patients. This is in agreement with a study by Esposito et al.25, which investigated the prevalence of depression in patients with whole age group with psoriasis and found 62% of patients to demonstrate depressive symptoms.
Although the prevalence of depression in our geriatric population with dermatological conditions was significantly higher than that of the general population, we have made some interesting observations. In the elderly population, it is well known that sociodemographic correlates of depression include female gender, divorced or separated marital status, low income and/or educational level, inadequate social support, and recent undesirable and unexpected life events26,27. In this study, lower education level was indeed a risk factor for depression, although we were not able to identify other sociodemographic variables that independently predicted depression.
In a study of Korean geriatric population, Lee et al.28 reported that depression in the elderly was not associated with sociodemographic variables but, rather, was related to the presence of physical illness, stressful life events, and cognitive dysfunction. In other studies investigating the psychosocial burden of psoriasis and vitiligo, disease severity, disease extent, and visibility of the lesions were strong predictors of the psychological impairment22,24,29. The multiple regression analysis in this present study, however, found no significant differences between depressive and non-depressive groups when considering medical-history variables such as diagnosis, disease category, and disease duration.
The recruitment method of patients from our dermatological department was not without its limitations. Despite the high response rates, our patients may not represent the entire geriatric population with dermatologic conditions. First, the sample size was not large. Second, as a tertiary referral center, our clinic is visited by a greater number of patients with severe and/or intractable diseases than the norm, and this may have contributed to an over-representation of dermatologic patients under increased psychological burden. However, the analysis of disease categories in our study closely resembles known clinical pattern of skin diseases in the general geriatric population30,31. This implies that our sampling could be considered representative of the general distribution of geriatric dermatological conditions. From this perspective, the potential selection bias appears to be minimal in this study.
Another limitation of the study design was in the self-administered nature of the survey. In contrast to questions of objective nature (i.e. demographic information such as age and gender), questions concerning disease characteristics were inherently liable to subjective interpretations and to potential misinterpretation by the patient. With the elderly population growing worldwide, geriatric depression is a major health concern that can be life threatening if not recognized in time and properly managed. This is a disease that significantly reduces quality of life and also is the single most important predictor of suicide27. In particular, physical health has a major impact on a person's mood and well-being, and geriatric skin disorders often represent a symptom or complication of an underlying systemic disease. According to Koenig and Blazer26, the rate of major depressive disorder in the hospitalized elderly patients is over 10 times the rate reported for the general population. In univariate analysis, our results were consistent with such studies in showing that physical health and certain systemic diseases correlated significantly with a higher GDS score. The concurrent disease included allergic rhinitis, angina, arrhythmia, asthma, benign prostate hyperplasia, cerebral vascular accident, congestive heart failure, dementia, dyslipidemia, gastritis, gastroesophageal reflux disease, gout, herniated nucleus pulposus, osteoarthritis, osteoporosis, rheumatoid arthritis, thyroid disease, tuberculosis, and varicose veins.
In the presence of a skin disorder, patients experience physiological changes that are induced by the mental stress, and these two factors feed each other in a vicious cycle. Most skin diseases in the elderly are chronic and recurring and incurs higher healthcare utilization costs. As a consequence, these patients may suffer from an increased rate of depression secondary to the psychological impact of the ongoing, long-term treatment. Thus, accurate and early diagnosis of depression is important because depression is a substantial morbidity which can be ameliorated with a variety of pharmacological and nonpharmacological interventions32,33.
In conclusion, geriatric patients with dermatological diseases are at an increased risk of depression. The results of this study should draw the attention of any physician who manages elderly patients with dermatologic diseases, as appropriate screening for depression and provision of emotional support are likely to improve the prognosis for the patient. Further investigation into the relationship of dermatologic diseases and depression in the elderly should determine the mechanisms by which dermatological disease is associated with higher rates of depression as well as approaches to prevent adverse psychological outcomes in the elderly with skin disorders.
In this preliminary study, we did not actively manage the psychological aspects of those patients with high GDS scores. It is possible that more active interventions, such as antidepressants prescription and psychosocial support, would reduce stress and depression32,33 and subsequently improve the prognosis of skin disease. Considering the increased rate of depression in this population, we hope to test the hypothesis above by performing an active psychological intervention in a future study.



 XML Download
XML Download