

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Linear focal elastosis (LFE) was first described by Burket et al.1 in 1989 in three elderly men. Since then, only 24 cases of LFE have been described in the English literature. Analysis of the reports currently available confirm male predominance, while the typical age of onset remains less clear2. A distinct clinical picture of the condition is marked by the occurrence of several asymptomatic, yellow, palpable, irregularly indurated, striae-like lines extending horizontally across the middle and lower back2. A focal increase in elastic fibers is a hallmark of the disease as seen from biopsy specimens1.
CASE REPORT
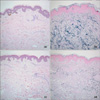
A 15-year-old male patient presented with multiple yellow, elevated, palpable, irregularly indurated linear plaques on the lower third of his back and several reddish depressed linear patches on the middle portion of his back (Fig. 1). The patient first noticed the elevated plaques nearly 5 years prior to presentation, and at that time, he had rapidly increased in height (growth spurt). The depressed patch lesions were observed 2 years prior to presentation. The number of linear plaques had slightly increased during that time. The patient had no relevant medical history of systemic or topical drug use. Two biopsy specimens were taken from the elevated plaques and depressed patches on the patient's back. The elevated plaque specimens showed focally thick collagen (Fig. 2a). Verhoeff-van Gieson staining demonstrated an increased amount of elastic fibers characterized by wavy, fragmented, and agglutinated elastic fiber bundles (Fig. 2b). The depressed patch specimens showed mild atrophic epidermis, edematous loose collagen bundles (Fig. 2c), and diminished elastic fibers (Fig. 2d). Therefore, he was diagnosed with LFE and SD.
DISCUSSION
The pathogenesis of LFE is still unclear, as is the association between LFE and SD. SD is distinguished by clinical and histopathologic features from LFE, such as depressed lines or bands of thin, reddened skin, which later become white, smooth, shiny, and depressed3. The main histopathologic feature of SD is epidermal atrophy, ruptured collagen bundles, dilation of dermal vessels and diminished elastic content2. Therefore, some authors have suggested that LFE is an independent disorder from SD1,4.
However, three published cases reported a concomitant finding of LFE and SD5-7. Generally, in later stages of SD, following the period of diminished elastic content, a regenerative phase occurs, during which de novo synthesis of elastic fibers increases2. Therefore, the prevailing opinion was that the association of LFE with SD could not be excluded. LFE represents an excessive regenerative process of elastic fibers and therefore could be considered to represent keloidal repair of SD5.
In conclusion, our case is the fourth known case of concomitant LFE and SD, and the second case in which LFE and SD were present at the same locations. Although the timing of LFE and SD onset was not synchronous in our patient, the triggering factor was the same, which was the growth spurt. This case supports the putative association between LFE and SD. However, to further explore this association, more studies with larger numbers of subjects are required.

 XML Download
XML Download