

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Basal cell carcinoma (BCC) is now frequently treated with photodynamic therapy (PDT), because of favorable treatment response and cosmetic outcome1. However, it is less effective in nodular BCC than in superficial BCC due to limited penetration of the photosensitizer. We recently successfully treated a thick lesion of classic Kaposi sarcoma with intralesional 5-aminolevulinic acid (ALA) injection PDT2. Intralesional injection (ILI)-PDT has also been tried in various cutaneous diseases with good clinical outcomes3. To our knowledge only one case of nodular BCC treated with 5-ALA ILI-PDT has been reported4. Herein, we report another case of nodular BCC successfully treated with 5-ALA ILI-PDT after a relatively short incubation time.
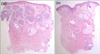
A 63-year-old man presented with a 1×0.8 cm-sized brownish papule with a rolled border on the right perinasal area, initially noted six months previously (Fig. 1a). Histopathological examination showed islands of atypical basaloid tumor cells with peripheral palisading, extending into the reticular dermis (Fig. 2a). In an attempt to treat the thick tumor with a shortened incubation time, we utilized 5-ALA ILI-PDT. Twenty-percent 5-ALA solution (Levulan Kerastick®; DUSA Pharmaceuticals, Wilmington, MA, USA) was injected into the lesion (about 0.3 ml/cm2). After 90 minutes, it was irradiated with red light from a Waldman PDT 1200 L lamp (Herbert Waldmann GmbH & Co. KG, Villingen-Schwenningen, Germany) at a light dose of 100 J/cm2, a fluence of 100 mW/cm2 and an emission wavelength of 580 to 740 nm. PDT was delivered repeatedly five times, at two to eight week intervals over six months. During the treatment, there were no noticeable side effects except mild pain during injection. Upon the follow-up visit eight months after the initial treatment, the lesion was cleared, leaving a faintly erythematous scar on the treated site (Fig. 1b). Skin biopsy showed only signs of chronic dermatitis and fibrosis without abnormal tumor cells, confirming the remission histopathologically (Fig. 2b).
Previous trials of topical PDT in treatment of BCC have shown promising results1. However, insufficient uptake of the photosensitizer to deeply located tumor cells has sometimes led to poor response. To facilitate transcutaneous absorption, various methods of pretreatment were introduced, such as curettage, debulking, tape stripping, microdermabrasion and laser ablation5. These techniques may produce substantial bleeding, consequently washing off the photosensitizer applied superficially on the tumor. Sotiriou et al.3 suggested that the photosensitizer may penetrate the target tissue deeply enough if it is directly injected into the tumor itself. We agree with this idea, because ILI causes only minimal bleeding at the puncture site. It may also shorten the incubation time required before adequate absorption is achieved, since it allows direct infiltration into the tumoral tissue. Therefore, the long incubation time, one of the major drawbacks of topical PDT, could be reduced with ILI of the photosensitizer.
However, the cost and prolonged treatment time, compared with simple excision, would discourage the use of ILI-PDT in a small BCC lesion. Further studies of ILI-PDT in nodular BCC with larger lesions are warranted for the evaluation of treatment efficacy and recurrence.

 XML Download
XML Download