

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Although melanoma mortality has levelled in many countries, the incidence is still rising1. Metastatic melanoma is very resistant to standard treatment modalities, including chemotherapy and radiotherapy2. Since melanoma is known to be a very immunogenic tumour, various immune targeted therapies are under trial3. For local cutaneous melanoma metastasis, Rose Bengal, a water soluble xanthine dye, and intralesional bleomycin have been used and are under ongoing research4.
Diphencyprone (DPCP) is a contact sensitizer with immunomodulator effects, commonly used for alopecia areata and warts5. DPCP was reported as an effective treatment for the local cutaneous metastatic melanoma on its own6,7 and in combination with cimetidine8 or dacarbazine and radiation therapy9. However DPCP alone as a treatment for cutaneous metastatic melanoma was reported from only one center so far6,7. We present a case of metatstatic melanoma successfully treated with DPCP.
A fifty seven year old Caucasian male presented with multiple enlarging asymptomatic pink nodules on his right shin for 6 months. He had superficial spreading malignant melanoma of Breslow thickness 1.20 mm, Clark level 4 excised from his right ankle 6 years prior.
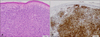
On examination, he had multiple erythematous superficial and deep nodules on right shin ranging in size from 5 to 25 mm. Histological examination of the lesions confirmed melanoma, consistent with metastatic melanoma. Subsequent pelvic computed tomography scan and positron emission tomography scan showed no evidence of distant metastasis. Based upon the impression of metastatic melanoma limited to local spread, he was started on DPCP therapy. Intralesional interferon and radiation therapy were considered not suitable due to the cost, location, and extent of the disease.
Initially he was sensitized with 2% DPCP in acetone in right inner upper arm. Two weeks later, he was started on 0.005% DPCP in aqueous cream weekly on the whole surface of right shin. He was instructed not to wash the area for 48 hours after the DPCP application. Subsequently the concentration of DPCP was increased to 0.01% for 3 weeks then 0.03% thereafter in order to achieve 2 to 3 days of eczematous reaction.
On examination after 18 weeks of weekly DPCP application, his right shin showed moderate dry eczematous changes with no evidence of nodules. Further histological examination from the two sites of the previous nodules revealed marked spongiosis with numerous eosinophils, consistent with allergic contact dermatitis, but no evidence of melanoma. The patient has continued on the weekly 0.03% DPCP. The patient tolerated the treatment very well with no notable side effects.
A previously reported case series showed variable response to DPCP among seven patients7. Later Th17 up-regulation was implicated as a mechanism for the regression of metastatic melanoma by DPCP10. However this was based on Th17 expressions of before and after treatment biopsy specimens from a single patient. Further studies are needed to characterize patients who will respond to DPCP therapy. Th17 expression was not studied in our case.
It is not clear how long the treatment should continue once the metastatic melanoma clears. There are not enough cases to assess the response rate and survival benefits. Since DPCP is a relatively very cheap, safe and easily accessible medication, further trials from various centers would be warranted. DPCP should be considered by the clinicians as a treatment option for the patient with cutaneous metastatic melanoma with no distant metastases.



 XML Download
XML Download