

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiac myxoma, although rare, is the most common primary cardiac tumor1. Approximately 75% of myxoma occurs in the left atrium during an individual's 30s to 60s, and it occurs more commonly in women2. Although these tumors are pathologically benign, they can clinically be considered malignant, especially when the tumor obstructs intracardiac blood flow, has embolic effects, or both3. About half of embolisms, which may occur in one-third of patients with cardiac myxoma, go to the brain, while others develop into cutaneous lesions.
Symptoms of embolization include cyanosis, especially of the fingers, which usually show color changes upon pressure or with cold or stress, petechiae, erythematous papules, and plaques with pruritus on the palm.
We report an interesting case of a 42-year-old male patient with cardiac myxoma diagnosed by multiple purpuric macules on the both palms and soles.
CASE REPORT
A 42-year-old male patient was transferred from the hematology department to the dermatology department for evaluation of purpuric lesions on both palms that had developed 2 weeks prior. He presented with 3 episodes of acral purpuric macules that had resolved within several weeks accompanied by malaise and fatigue. Initial symptoms started 4 months before hospitalization. He was in a good general health prior to the initial attack and had no history of drug abuse, thoracostomy, or congenital heart disorders.
Physical examination revealed multiple tender purpuric macules on both palms and soles (Fig. 1). Laboratory tests, including complete blood cell count, liver function test, blood coagulation test, serology for treponematosis (venereal disease research laboratory, treponemal pallidum particle agglutination), antinuclear antibody, and muscle enzymes were negative or within normal limits.
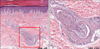
The patient was first believed to have vasculitis, for which a biopsy was performed on the left palm. Histopathological findings revealed a myxomatous embolus in the arteriole of the lower dermis (Fig. 2).
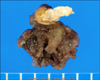
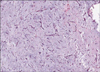
With this finding, cutaneous embolization of cardiac myxoma was suspected and an echocardiogram was performed, which demonstrated the presence of a large left atrial mass (Fig. 3). A provisional diagnosis of a left atrial myxoma was made. Emergency open heart surgery was performed and the tumor was excised (Fig. 4). The patient made a complete recovery without additional complications. Postoperative pathological findings confirmed the diagnosis of cardiac myxoma (Fig. 5).
The cutaneous lesions resolved within 1 week after the operation. No more similar cutaneous lesions or systemic symptoms including intra- or extracardiac obstructive signs such a heart failure, cerebrovascular accident, or cardiovascular disease appeared, and a follow-up echocardiogram revealed no evidence of tumor recurrence for 5 years.
DISCUSSION
The clinical features of cardiac myxoma are based on its location, size, and mobility and can be morphologically variable. However, almost patients with this condition present with one or more clinical manifestations of the classic triad: 1) intracardiac obstructive signs; 2) extracardiac embolic signs; or 3) constitutional or systemic manifestations1.
First, intracardiac obstructive signs occurred in 67% of cardiac myxoma patients4. Progressive congestive heart failure (dyspnea, orthopnea) was the most common symptom (64%). Second, extracardiac embolic signs were seen in about one-third of patients. Approximately half of all embolic sites were within the central nervous system. Third, systemic symptoms, including fever, myalgia, arthralgia, or Raynaud's phenomenon, were present in 90% of patients5.
Cutaneous aspects of cardiac myxoma are usually non-specific and can be classified into 3 subtypes: 1) embolic cutaneous signs; 2) non-embolic cutaneous signs associated with auto-immune symptoms; and 3) cutaneous signs of a complex syndrome. First, embolic cutaneous signs resulting from fragmentation or complete tumor detachment occur in approximately 30~40% of cases. Tough myxomatous embolisms, which can affect any part of the arterial bed and involve the cerebral circulation in about 50% of cases, result in cerebrovascular accidents. In addition, embolization to the lungs, coronary arteries, kidneys, spleen, intestines, and extremities also occurs. According to Pinede's study, peripheral (limb) embolizations were present in 13% of patients4. They may appear as acral erythematous papular eruptions, telangiectasia, petechiae, splinter hemorrhages, and livedo reticularis3 and be episodic or recurrent. Sometimes they may progress into digital cyanosis and necrosis as a result of an ischemic condition caused by obstruction of blood circulation resulting from embolization. The histopathological findings were based on the presence of characteristic myxoma cells surrounded by an amorphous myxoid matrix that consisted of an acid-mucopolysaccharide-rich stroma. In our patient, the postoperative specimen showed myxoma cells scattered throughout the matrix that had a spindle or stellate shape, an ovoid nucleus, and an eosinophilic cytoplasm. These features disappear when the tumor is eliminated6.
Second, cutaneous features may be associated with autoimmune symptoms including Raynaud's phenomenon, malar erythema, and vasculitis, which can be explained by myoxomal secretion of interleukin-67. These symptoms usually disappear after removal of the cardiac myxoma, although prolonged elevation of antinuclear antibodies has been noted8.
Third, some cutaneous findings suggest the diagnosis of cardiac myxoma as part of a more complex syndrome. Nevus, atrial myxoma, myxoid neurofibromas, and ephelides as well as lentigines, atrial myxoma, and blue nevi have been described9, and a subsequent report has described Carney syndrome, which is characterized by autosomal dominant transmission, myxoma, spotty pigmentation, endocrine overactivity, and schwannomas10.
The differential diagnosis of the cutaneous findings of cardiac myxoma consists of several diseases including vasculitis, livedo reticularis, and pigmented purpuric dermatosis.
To the best of our knowledge, 4 cases of cardiac myxoma associated with cutaneous manifestations have been reported in the Korean medical literature3,9,11,12. Of these 4 previously described patients, one was related to migratory erythematous maculopapules, another was associated with pseudovasculitis, and the others presented with livedo reticularis.
Because the tumor's histological benignancy contrasts with its malignant clinical behavior in terms of systemic embolization, early diagnosis and surgical intervention are essential. However, cardiac myxoma illustrates that this benign tumor may cause a broad spectrum of clinical manifestations including not only cardiac disease but also infective, immunologic, or neurologic diseases. Also, it has no specific or pathognomic signs or symptoms. Therefore, clinical diagnosis of cardiac myxoma remains difficult, especially when cardiac symptoms are not present as in our patient. In this case, the skin lesions were the first sign of the disease and may play a very important role in the diagnosis of a patient with cardiac myxoma.
In conclusion, this case of cardiac myxoma diagnosed by the presence of purpuric macules on both palms and soles emphasizes to clinicians that cutaneous manifestation can be an important clue in the prompt diagnosis and early intervention. Therefore, although it is uncommon, cardiac myxoma should be considered when the cutaneous findings described above are observed in a patient, so dermatologists must recognize the various cutaneous findings associated with it.


 XML Download
XML Download